|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 2 | Page : 63-66 |
|
Pattern of presentation of dermatomycosis in diabetic patients in Aba, South-eastern, Nigeria
AC Ngwogu1, KO Ngwogu2, IEK Mba3, EC Uchefuna3, TV Otokunefor4
1 Department of Medical Microbiology and Immunology, College of Medicine and Health Sciences, Abia State University, Uturu, Abia State, Nigeria
2 Department of Chemical Pathology, College of Medicine and Health Sciences, Abia State University, Uturu, Abia State, Nigeria
3 Department of Internal Medicine, Faculty of Clinical Medicine, College of Medicine and Health Sciences, Abia State University, Uturu, Abia State, Nigeria
4 Department of Microbiology, Faculty of Science, University of Port Harcourt, Rivers State, Nigeria
| Date of Web Publication | 19-Aug-2014 |
Correspondence Address:
A C Ngwogu
Faculty of Clinical Medicine, College of Medicine and Health Sciences, Abia State University, Uturu, Abia State
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/9783-1230.139164

Background: Dermatomycoses, although a common health problem amongst diabetics, is often misdiagnosed and consequently undertreated. Objective: The aim was to obtain information on the pattern of dermatomycoses in diabetics in Aba, Abia State, Nigeria. Design: Data sources from patients attending diabetic clinics in three major hospitals in Aba, Abia State, Nigeria. Setting: Abia State University Teaching Hospital, Living Word Hospital, and New Era Hospitals, all in Aba, Abia State, Nigeria. Materials and Methods: A total of 400 diabetic patients were recruited for this study. Results: A total of 97 (24.3%) diabetics had lesions suspected to be dermatomycoses and dermatophytoses was the most common infection observed. Others are candidiasis and pityriasis. Trichophyton mentagrophytes was the most frequently isolated fungal organism. Lesions occurred more often at the inguinal region. Fasting blood sugar (FBS) levels ranged from 6.6 to 20.3 mmol/L. The prevalence of dermatomycoses was higher in diabetics with poor metabolic control. Conclusion: Fungal skin infections are common in diabetics, especially in those with poor control. Keywords: Aba, Dermatomycoses, Diabetics, Nigeria
How to cite this article:
Ngwogu A C, Ngwogu K O, Mba I, Uchefuna E C, Otokunefor T V. Pattern of presentation of dermatomycosis in diabetic patients in Aba, South-eastern, Nigeria. J Med Investig Pract 2014;9:63-6 |
How to cite this URL:
Ngwogu A C, Ngwogu K O, Mba I, Uchefuna E C, Otokunefor T V. Pattern of presentation of dermatomycosis in diabetic patients in Aba, South-eastern, Nigeria. J Med Investig Pract [serial online] 2014 [cited 2018 Aug 24];9:63-6. Available from: http://www.jomip.org/text.asp?2014/9/2/63/139164 |
| Introduction | |  |
Dermatomycoses are diseases of the skin or its appendages caused by fungi. Among these are dermatophytoses, candidiasis, piedra, pityriasis, tinea nigra, onychomycoses and paronychomycosis. [1] The skin serves as a barrier and prevents the invasion of the body by microorganisms. The factors that enable the skin to carry out this function include the skin structure, constant shedding of epidermal cells, fatty acid content and pH. [2] Fungal spores however colonize the skin when these natural barriers are compromised and deeper epidermal layers are not able to activate the immune response.
Diabetes mellitus is a chronic clinical syndrome characterized by hyperglycaemia due to deficiency of or defective response to insulin. [3] Diabetes mellitus is classified into Type 1, insulin dependent diabetes mellitus (IDDM) and Type 2, non-IDDM (NIDDM) based on the chemicals, etiopathogenic and pathophysiological mechanisms involved. IDDM occurs, as a result, of some environmental factors initiating the autoimmune destruction of B cells of Islets of Langerhans More Details. This leads to reduced insulin production in genetically susceptible individuals. [4] NIDDM occurs either, as a result, of target cells not responding to available insulin (i.e. insulin resistance) or a delayed insulin secretion relative to glucose level. [5],[6] Diabetes mellitus is usually associated with numerous skin alterations that may develop due to these metabolic and structural disturbances making the skin more susceptible to colonization by fungi. One of such alterations is the increased skin sugar level. [7] Another is the immune response abnormality which is characterized by reduced neutrophil chemotaxis and phagocytosis. [8]
The prevalence and pattern of dermatomycoses among diabetics has been studied in other parts of the world. [3],[9],[10] There is no evidence of such studies in Nigeria. The present study is aimed at investigating the prevalence and etiology of dermatomycoses in diabetics in Aba, Abia State, Nigeria and the possible influence of metabolic control of diabetes mellitus on the prevalence of dermatomycoses.
| Materials and methods | | |
A total of 400 diabetics attending diabetic clinics in three major hospitals in Aba, Abia State, Nigeria, were examined for lesions of dermatomycoses. Positive lesions were cleaned with cotton swabs soaked in methylated spirit and scrapings were obtained using a clean scalpel. Each sample was properly labeled with name, sex, age and site of the body of the patient from where it was collected. Fasting blood samples were collected from patients with dermatomycoses to determine their fasting blood sugar (FBS) levels.
Microscopic examination of samples
Each samples was examined in a drop each of 10% potassium hydroxide solution and 40% dimethylsulfoxide for the presence of fungal structures and spores. [11]
Isolation and identification of isolates
A portion of each sample was cultured on sabouraud dextrose agar (SDA) supplemented with chloramphenicol and cycloheximide and on SDA with only chloramphenicol. Olive oil (2%) was added to the SDA without cycloheximide when pityriasis was suspected. The plates were incubated at 25°C or 30°C. Plates were examined daily for 4 weeks until fungal growth was observed. Filamentous fungi were identified using their macroscopic and microscopic characteristics. The slide culture technique was employed to better visualize the arrangement and shape of the spores for proper identification. Other tests employed to enhance identification are urease test, in-vitro hair perforation test, temperature tolerance test and the ability of the organisms to grow on polished rice. In addition to their macroscopic and microscopic characteristics the yeasts/yeast like isolates were identified using biochemical tests (sugar fermentation, sugar assimilation and germ tube production). All tests were carried out according to the methods specified in mycology manuals. [12],[13],[14]
Fasting blood sugar estimation
This was done by alkaline copper reduction method and recorded in millimole per liter. [15]
| Results | | |
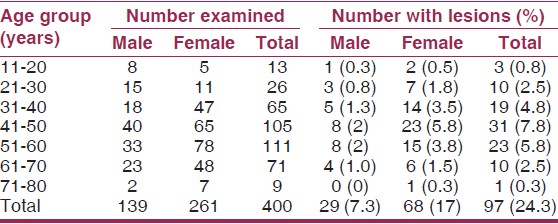
Out of the 400 diabetics examined; 139 were males and 26 females. A total of 97 (24.3%) had lesions consistent with dermatomycycoses. Dermatophytoses accounted for 66.6% of the fungal infections, candidiases 24.1% and pityriasis, 9.2%. There was a significantly higher incidence of dermatomycoses in female diabetics compared to male diabetics (P < 0.05). The ages of the patients ranged from 17 to 76 years. The age and sex distribution of lesions are shown on [Table 1]. Pruritus was present in 15.5% of those with lesions.
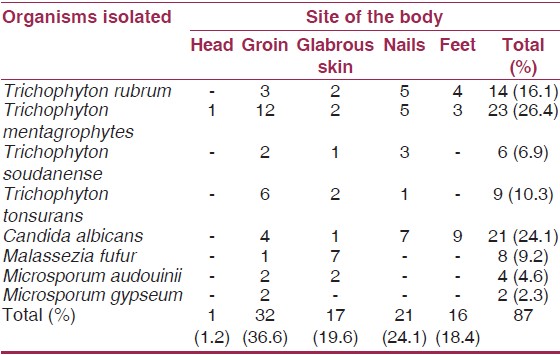
Fungal organisms were identified in 87 samples. Trichophyton mentagrophytes was the most frequently isolated agent and was isolated from 23 cases (26.4%). Other organisms isolated included Trichophyton rubrum (16.1%), Trichophyton soudanense (6.9%), Trichophyton tonsurans (10.3%), Candida albicans (24.1%), Malassezia furfur (9.2%), Microporum audouinii (4.6%) and Microsporum gypseum (2.3%). The distribution of the organisms according to the area of the body affected is shown on [Table 2].
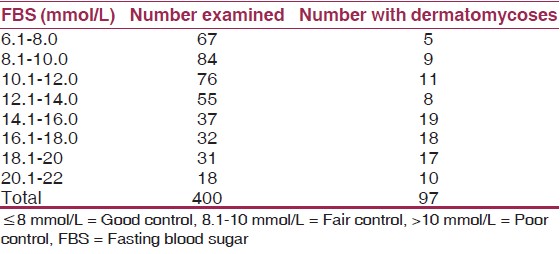
Among the diabetics studied, 39 were of the IDDM while 361 were of NIDDM. The duration of diabetes ranged from 1 month to 20 years. Average duration was 8 years 4 months. FBS levels ranged from 6.6 to 20.3 mmol/L (average was 10.2 mmol/L). The prevalence of dermatomycoses was higher in diabetics with poor metabolic control as shown in [Table 3].
| Discussion | | |
Studies on the prevalence and pattern of dermatomycoses in diabetics have been carried out in other parts of the world with incidence rates ranging from 1.4% to 75%. [9],[10],[16] The prevalent rate in this study was 24.3%. Dermatomycoses are not common in healthy adult populations. Childhood infections heal spontaneously at puberty. [1] In order to colonize the skin, fungal spores need to cross the natural barrier created by this keratinous, corneal layer. This requires possessing keratinase, overcoming the fungistatic action of fatty acids produced by the keratin cells and evading the immune response activated by deeper epidermal cells. [9] Phagocytsis, myeloperoxidase activity and leukocyte chemotaxis are impaired in the skin of diabetics thus exposing them to colonization by superficial fungi. [6],[17] This could explain the high incidence of infection obtained in the study population. In addition, the hot and humid climate of our setting could contribute to this high incidence of dermatomycoses observed. [18]
The present study showed that dermatomycoses were prevalent in all the age groups studied. This is similar to result obtained in a study carried out in India. [19] However, infection was most prevalent in the 20-30 years age group. This is due to a higher number of patients in this age group having decreased metabolic control, rather than age.
Infection was significantly higher in females than males. This is most likely due to the habit of women applying assorted body lotions that keep their bodies moisturised. In addition, their frequent use of bleaching creams that erode the skin and make it more susceptible to infection cannot be overlooked. [7]
Dermatophytoses, pityriasis and candidiasis were observed in the diabetics under study. Pityriasis was not observed among diabetics in India. [10] However, candidiasis is a common opportunistic infection that has been observed in diabetics. [9],[10],[19]
The most prevalent causative organism was T. mentagrophytes, a dermatophyte. T. rubrum was the most prevalent organism isolated from diabetics in Puerto Rico. [9] Differences in the causative organisms isolated in different studies may depend on the organisms prevalent in a particular area at a particular time. T. mentagrophytes has frequently been isolated from dermatophytoses in children in Aba, Abia State, Nigeria. [18] The spectrum of the organisms is causing dermatomycoses from place to place and even in the same place changes with time. [1] Lesions were seen more in the groins. This is probably because the area is covered with clothing most of the time and moisture builds up at the folds. Fungi thrive well in humid conditions. [18]
The FBS levels were used to estimate the level of metabolic control among the diabetics. The higher prevalence of dermatomycoses among diabetics with poor metabolical control agrees with other similar studies. [9],[10],[17] There is a need to emphasize the importance of regular check-ups and blood sugar monitoring to diabetics. This would increase their awareness of the implications of poor metabolic control.
In view of the fact that infection was detected in few diabetics with good metabolic control, it seems that though poor metabolic control is a major factor, it might not be the only factor predisposing to dermatomycoses in diabetics. Further studies need to be carried out to determine other factors that could play a role in the incidence of dermatomycoses among diabetics.
There is also a need for proper diagnosis and prompt treatment of dermatomycoses in diabetics to avoid the disruption of skin integrity, thus providing an avenue for bacterial superinfection. [7] In addition, these infections if not treated can get deeper than the skin surface causing life-threatening complications. [20],[21]
| Acknowledgments | | |
The authors are grateful to the Management and Staff of Living Word Mission Hospital, New Era Hospitals and Abia State University Teaching Hospital, all in Aba, Abia State, Nigeria for allowing us use their diabetic clinics
| References | | |
| 1. | Nelson MM, Martin AG, Heffernan MP. Superficial fungal infections: Dermatophytoses, Onychomycosis Tinea nigra, Piedra. Fungal diseases with cutaneous involvement In: Fitpatrick's Dermatology in General Medicine. 6 th ed. New York: McGraw Hill; 2003. p. 1989-2005. 
|
| 2. | Hainer BL. Dermatophyte infections. Am Fam Physician 2003;67:101-8.
|
| 3. | Romano C, Massai L, Asta F, Signorini AM. Prevalence of dermatophytic skin and nail infections in diabetic patients. Mycoses 2001;44:83-6.
|
| 4. | Eisenbarth GS. Type I diabetes mellitus. A chronic autoimmune disease. N Engl J Med 1986;314:1360-8.
|
| 5. | De Fronzo RA. Ferrannini E. Insulin resistance: A multifaceted syndrome responsible for type 2 diabetes mellitus, obesity, hypertension, dyslipidemia and artherosclerotic cardiovascular disease. Diabetes Care 1991;14:173-94.
|
| 6. | Bub JL. Olerud JE. Diabetes mellitus. In: Fitzpatrick's Dermatology in General Medicine. 6 th ed. New York: McGraw Hill; 2003. p. 1651-61.
|
| 7. | Urbach K, Lentz JW. Carbohydrate metabolism and the skin. Arch Dermatol Syphilol 1965;52:301-4.
|
| 8. | Delamaire M, Maugendre D, Moreno M, Le Goff MC, Allannic H, Genetet B. Impaired leucocyte functions in diabetic patients. Diabet Med 1997;14:29-34.
|
| 9. | Lugo-Somolinos A, Sánchez JL. Prevalence of dermatophytosis in patients with diabetes. J Am Acad Dermatol 1992;26:408-10.
|
| 10. | Nigam PK, Pande S. Pattern of dermatoses in diabetics. Indian J Dermatol Venereol Leprol 2003;69:83-5.
[PUBMED]  |
| 11. | Singh S, Beena PM. Comparative study of different microscopic techniques and culture media for the isolation of dermatophytes. Indian J Med Microbiol 2003;21:21-4.
[PUBMED] |
| 12. | Rebel G. Taplin D. Dermatophytes: Their recognition and identification Reversed ed. Florida: University of Miami Press; 1974.
|
| 13. | Larone DH. Medically Important Fungi: A Guide to Identification. 3 rd ed. Washington: ASM Press; 1995.
|
| 14. | Chaudra J. A Textbook of Medical Mycology. New Delhi: Melita Publishers; 1996.
|
| 15. | Cheesebrough M. District Laboratory Practice in Tropical Countries. Part 1. Cambridge: Cambridge University Press; 2005. p. 310-92.
|
| 16. | García-Humbría L, Richard-Yegres N, Pérez-Blanco M, Yegres F, Mendoza M, Acosta A, et al. Superficial mycoses: Comparative study between type 2 diabetic patients and a non-diabetic control group. Invest Clin 2005;46:65-74.
|
| 17. | Tan JS, Joseph WS. Common fungal infections of the feet in patients with diabetes mellitus. Drugs Aging 2004;21:101-12.
|
| 18. | Okafor JI, Agbugbaeruleke AK. Dermatophytoses among school children in Aba, Abia State - Nigeria and some physiological studies on the isolated etiologic agents. J Commun Dis 1998;30:44-9.
|
| 19. | Parthiban K, Janaki C, Sentamil SG, Janaki VR. Dermatomycoses in diabetics - A clinical study. Indian J Dermatol 1998;43:50-2.
|
| 20. | Erbagci Z. Deep dermatophytoses in association with atopy and diabetes mellitus: Majocchi's granuloma tricophyticum or dermatophytic pseudomycetoma. Mycopathologia 2002;154:163-9.
|
| 21. | Hohaus K, Vennewald I, Wollina U. Deep mycoses caused by Trichophyton mentagraphytes in a diabetic patient. Mycoses 2003;46:337.
|
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for