|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 2 | Page : 55-58 |
|
The burden of preterm births in Aba, Southeastern Nigeria
B Chigbu, S Onwere, C Aluka, C Kamanu, P Feyi-Waboso, O Okoro
Department of Obstetrics and Gynaecology, Abia State University Teaching Hospital, Aba, Nigeria
| Date of Web Publication | 19-Aug-2014 |
Correspondence Address:
S Onwere
Department of Obstetrics and Gynaecology, Abia State University Teaching Hospital, PMB 7004, Aba
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/9783-1230.139162

Background: Preterm birth is an important cause of perinatal mortality and morbidity in developing countries. Objective: To determine the burden of preterm birth in Aba, Southeastern Nigeria. Materials and Methods: A review of all preterm deliveries at the maternity hospital annex of the Abia State University Teaching Hospital, Aba, Nigeria between January 1, 2002 and December 31, 2006 was performed. Results: During the studied period, 5566 women delivered at the hospital. Three hundred and ninety-three of them had preterm birth, giving a preterm birth delivery rate of 7.1% in the hospital. Majority of the women, 229 (58.2%) had late preterm birth. Iatrogenic delivery was responsible for the preterm deliveries in 59 (15%) parturients. The mean of 1-min Apgar score was 5, while the mean of 5-min Apgar score was 7. The mean birth weight of babies was 1700 g (range 550-2800 g) whilst the total number of preterm deaths was 157, giving a preterm mortality rate of 40%. Conclusion: Preterm birth is a burden in Aba, Southeastern Nigeria. Improved care of preterm babies and measures to reduce the burden of preterm birth are urgently needed. Keywords: Preterm birth, Rate, Southeastern Nigeria
How to cite this article:
Chigbu B, Onwere S, Aluka C, Kamanu C, Feyi-Waboso P, Okoro O. The burden of preterm births in Aba, Southeastern Nigeria. J Med Investig Pract 2014;9:55-8 |
How to cite this URL:
Chigbu B, Onwere S, Aluka C, Kamanu C, Feyi-Waboso P, Okoro O. The burden of preterm births in Aba, Southeastern Nigeria. J Med Investig Pract [serial online] 2014 [cited 2018 Aug 24];9:55-8. Available from: http://www.jomip.org/text.asp?2014/9/2/55/139162 |
| Introduction | |  |
The main burden of preterm birth exists in developing countries. There are no accurate recent worldwide data, but estimates of preterm birth rates range from 5% in developed countries to 25% in developing countries. [1] Worldwide, an estimated 15 million babies are born preterm every year, and around 1 million children die each year due to complications of preterm birth. [1] In Nigeria, preterm birth rate has been on the increase and is currently 12/100 live births with prematurity accounting for 33% of neonatal deaths translating to about 87,800 deaths and 50% of long-term neurological impairment in children. [1] Many survivors, therefore, face a lifetime of disability, including learning disabilities and visual and hearing problems and create a huge burden for families, society and health-care system.
Whereas studies have shown that more than three-quarters of premature babies can be saved with feasible, cost-effective care [2] - e.g. antenatal steroid injections (given to pregnant women at risk of preterm labor to strengthen the babies' lungs), kangaroo mother care (the baby is carried by the mother with skin-to-skin contact and frequent breastfeeding) and antibiotics to treat newborn infections - even without the availability of neonatal intensive care; the survival of these preterm infants is still dependent on the function of their biological maturity and technological advancement where they are born. A previous study in Nigeria recorded a mortality of 92.6% in babies <28 weeks gestational age. [3]
Studies have demonstrated significant ethnic variation in preterm birth rates; with higher rates in black women. [4] This is associated with an accelerated rate of maturity in the black fetus and neonate. [5] Ethnic differences, however, can explain only a very small proportion of global preterm births. The greatest etiological factor worldwide is infection mainly due to malaria and HIV. [6] Nigeria has the second largest number of people living with HIV and AIDS.
The aim of this study is to determine the burden of preterm birth in Aba, Southeastern Nigeria. It is hoped that the findings in this study will help identify in our antenatal clinics the women at risk of preterm deliveries and who may therefore benefit from interventions that prevent these deliveries. It is also hoped that this study will help raise awareness for this public health problem in our community.
| Materials and methods | | |
A review of all preterm deliveries at the maternity hospital wing of the Abia State University Teaching Hospital, Aba, Nigeria between January 1, 2002 and December 31, 2006 was performed. This wing of the hospital provides secondary and tertiary health-care services in obstetrics and gynecology. It attends to both booked and unbooked emergencies. The annual delivery rate is between 1000 and 1500. The neonatal intensive care unit provides care to both inborn and outborn neonates. It admits between 800 and 1200 neonates annually.
The case records of the patients were obtained from the central delivery unit and the medical records department and analyzed to determine the proportion of parturients that had preterm delivery. All recorded cases of preterm delivery between 2002 and 2006 were reviewed. The data obtained were analyzed using simple proportion, rates and tables. Ethical clearance was obtained from the Ethics and Research Committee of the Abia State University Teaching Hospital, Aba, Nigeria.
| Results | | |
During the studied period, 5566 women delivered at the hospital. Three hundred and ninety-three of them had preterm birth, giving a preterm birth delivery rate of 7.1% in the hospital, [Table 1] with some slight annual increase.
Majority of the women, 229 (58.2%) had late preterm birth, 55 (14.0%) had moderate preterm birth, 69 (17.6%) had very preterm birth, whilst 40 (10.2%) had extreme preterm birth. The sex distribution of the babies was 198 males and 195 females.
Iatrogenic delivery was responsible for the preterm deliveries in 59 (15%) women due to hypertensive disorders, diabetes and intrauterine growth restriction. Spontaneous preterm labor was the cause in 334 (85%) parturients.
The mean of 1-min Apgar score was 5 while the mean of 5-min Apgar score was 7. Majority of the babies, 270 (68.2%) were asphyxiated as evidenced by the 1-min Apgar score of ≤6. The total number of preterm deaths was 157, giving a preterm mortality rate of 40%. Majority of the births, 230 (58.5%) occurred during the dry season (October to February), whilst 163 (41.5%) preterm births were during the rainy season (March to September).
The mean birth weight of babies was 1700 g (range 550-2800 g). Babies with low birth weight (≤2500 g) were 296 (75.3%).
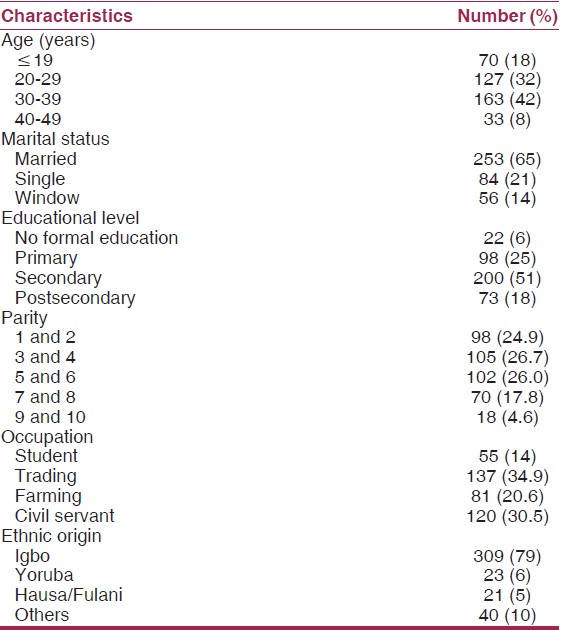
[Table 2] shows the sociodemographic characteristics of the women who had preterm birth. The mean age of the women was 30 years (range 17-45 years). Majority of the women, 253 (65%) were married. Eighteen percent were teenagers. The parity ranged between 1 and 10, with a mean of 4. Majority of the women having preterm birth were traders, 137 (34.9%).
The pregnancy complications associated with the preterm births included, premature rupture of the membrane in 14.8% of the women, malaria in 40.5%, antepartum hemorrshage in 10.4%, anemia in 20% of the women, hypertensive disorders in 7.4%, and high order multiple pregnancies in 2%. Others were fibroid coexisting with the pregnancy in 7.5% of the women, polyhydramnios in 6%, intrauterine growth restriction in 7.6% of the cases, gestational diabetes mellitus in 4% and HIV infection in 2% of the women. More than one complication was encountered in many of the women delivering preterm.
| Discussion | | |
This study reveals a preterm delivery rate of 7.1% at the Abia State University Teaching Hospital, Aba, Nigeria. Although this figure is lower than the national prevalence rate of preterm birth, it is slightly higher than the rate of 6.2% reported at the University of Benin Teaching Hospital. [3] This is worrisome in view of the paucity of neonatal intensive care units and personnel to take care of preterm babies in our locale. Majority of the preterm babies were low birth weight babies. The high overall preterm mortality rate amongst these babies is, therefore, not surprising as the hospital lacks modern facilities and personnel for neonatal intensive care. Majority of the babies were asphyxiated at birth and this is to be expected since the mean birth weight of the babies was as low as 1700 g. One can only imagine the social and emotional cost of the perinatal morbidity and mortality associated with preterm births in this hospital. Improved care is urgently needed, but would require a lot of technical and ancillary support that may not be easy to come by within the context of political instability and insecurity in Nigeria today.
In developed countries, iatrogenic delivery when there is a risk of fetal compromise is responsible for almost half of the preterm births between 28 and 35 weeks. [1] In this study iatrogenic delivery was responsible for 15% of the preterm births due to hypertension, diabetes and intrauterine growth restriction. The commonest complication associated with preterm delivery in the women was spontaneous preterm labor. Other observed complications were premature rupture of the membrane, malaria, antepartum hemorrrhage, anemia, and high order multiple pregnancies. Some women also had fibroid coexisting with the pregnancy, polyhydramnios, and HIV infection.
In sub-Saharan Africa, infectious morbidities are the single most common cause of preterm birth [6],[7],[8] and malaria is the most widely distributed of such diseases as 40% of pregnant women worldwide are exposed to malaria during pregnancy. [9] In a recent study in Malawi peripheral malaria parasitemia of the mother accounted for 65% of the population-attributed risk of perinatal mortality. [10] HIV has also been a problem in Africa. In 2010, the HIV prevalence rate in Nigeria was 4.1%. [11] This means that the number of people infected with HIV in Nigeria is 3.1 million.
Multiple pregnancy and higher order births are also major causes of preterm birth. West Africa has the highest incidence of naturally conceived multiple pregnancies in the world (1 in 40). [12]
Findings in this study indicate that there were more preterm babies in the dry season than in the rainy season in our locale. This differs from the observation at Benin. [5] This may be explained on the basis that majority of the women in this study were traders who may have been involved in much psychological stress and heavy physical work while combining their house chores with trading in the peak months of commerce in Aba, the commercial nerve center of Southeastern Nigeria. Heavy and stressful occupation is a known significant risk factor of preterm delivery. [13]
| Conclusion | | |
Preterm birth is a burden in Aba Southeastern Nigeria. Improved care of preterm babies and measures to reduce the burden of preterm birth are urgently needed. When there are antenatal complications such as malaria, anemia, hypertension, and HIV, preterm birth should be anticipated and strategies to reduce neonatal morbidity and mortality instituted where possible. Women with multiple pregnancy or high other multiples should be termed high risk for preterm birth.
There is a need to educate our women on the risks of high physical work and other maternal stress inducing factors during pregnancy. Healthy nutrition in pregnancy should also be encouraged. Intermittent treatment of malaria with sulfgadoxine-pyrimethamine in pregnancy should continue to receive encouragement. Pregnant women should be encouraged to sleep in insecticide treated bed nets.
| Limitations of the study | | |
There are few limitations in this study. The study was hospital based and a retrospective review. It was observed that the concept of "completed weeks" is still widely misunderstood. Many clinicians and midwives in the hospital were incorrectly using "rounding." Hence 36 weeks and 6 days of gestational age were sometimes recorded as 37 weeks or "term." Furthermore, the potential risk factors of preterm birth identified in this study were not subjected to multiple regression analysis to ascertain which factors would remain significant. This was because the review is a pilot study. There is need therefore for a more robust population based study in our locale to expand on the issues raised.
| References | | |
| 1. | Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012;379:2162-72. 
|
| 2. | WHO. Kangaroo Mother Care: A Practical Guide. Geneva: WHO; 2003. Available from: http://www.mamaye.Org/evidence/kangaroo-mother-care-practical guide. [Last accessed on 2014 Feb 22].
|
| 3. | Ibhanesebhor SE, Afadapa MA. Epidemiology of preterm delivery in Benin City. Niger J Paediatr 1996;23:27-32.
|
| 4. | Patel RR, Steer P, Doyle P, Little MP, Elliott P. Does gestation vary by ethnic group? A London-based study of over 122,000 pregnancies with spontaneous onset of labour. Int J Epidemiol 2004;33:107-13.
|
| 5. | Allen MC, Alexander GR, Tompkins ME, Hulsey TC. Racial differences in temporal changes in newborn viability and survival by gestational age. Paediatr Perinat Epidemiol 2000;14:152-8.
|
| 6. | Ayisi JG, van Eijk AM, ter Kuile FO, Kolczak MS, Otieno JA, Misore AO, et al. The effect of dual infection with HIV and malaria on pregnancy outcome in western Kenya. AIDS 2003;17:585-94.
|
| 7. | Ticconi C, Mapfumo M, Dorrucci M, Naha N, Tarira E, Pietropolli A, et al. Effect of maternal HIV and malaria infection on pregnancy and perinatal outcome in Zimbabwe. J Acquir Immune Defic Syndr 2003;34:289-94.
|
| 8. | Etuk SJ, Etuk JS, Oyo-Ita AE. Factors influencing the incidence of pre-term birth in Calabar, Nigeria. Niger J Physiol Sci 2005;20:63-8.
|
| 9. | Shulman CE, Dorman EK. Importance and prevention of malaria in pregnancy. Trans R Soc Trop Med Hyg 2003;97:30-5.
|
| 10. | Kulmala T, Vaahtera M, Ndekha M, Koivisto AM, Cullinan T, Salin ML, et al. The importance of preterm births for peri - And neonatal mortality in rural Malawi. Paediatr Perinat Epidemiol 2000;14:219-26.
|
| 11. | National HIV Sero-Prevalence Sentinel Survey 2010. Available from: http://www nigera-aids.org/…/2010. [Last accessed on 2014 Feb 12].
|
| 12. | Onyiriuka AN. Twin delivery incidence and perinatal outcome in a Nigerian Mission Hospital. Bangladesh J Med Sci 2011;10:45-51.
|
| 13. | Ezechi OC, Makinde ON, Kalu BE, Nnatu SN. Risk factors for preterm delivery in South western Nigeria. J Obstet Gynaecol 2003;23:387-91.
|
[Table 1], [Table 2]
|









 Search Pubmed for
Search Pubmed for