|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 3
| Issue : 2 | Page : 141-145 |
|
Nonextraction management of the labially displaced canine
Zeeshan Iqbal Bhat1, Charu Dutta Naik2
1 Departments of Orthodontics and Dentofacial Orthopedics, Dahim Medical Center, Al Ahsa, Eastern Province, Saudi Arabia, Saudi Arabia
2 Dr. D.Y. Patil Dental College and Hospital, Pimpri, Pune, Maharashtra, India, India
| Date of Web Publication | 15-May-2015 |
Correspondence Address:
Zeeshan Iqbal Bhat
Dahim Medical Centre, Al-Ahsa, Eastern Province, Saudi Arabia
Saudi Arabia
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.150570

Maxillary canine impaction is an anomaly often encountered in children. Although it has been reported that the incidence of palatally impacted canines is higher than that of labially impacted ones, it has been found that labial impaction of canines is more common than palatal impaction in Asian populations. Bringing the ectopic canine into a normal position is important for functional occlusion and the final esthetics of the orthodontic treatment. This article represents a nonextraction treatment approach for a labially displaced canine of a young boy, aged 12 years 6 months, with maxillary transverse discrepancy, labially placed maxillary canine, cross bite with UL3, UL4, UL5, midlines discrepancy, severe crowding in mandibular arch. The orthodontic treatment plan included slow palatal expansion followed by fixed orthodontics which guided the maxillary canine into the arch. This treatment strategy achieved optimal occlusion with improvements to the transverse, vertical, and sagittal relationships and achieved a harmonious smile. Keywords: Impaction, maxillary canine, slow maxillary expansion
How to cite this article:
Bhat ZI, Naik CD. Nonextraction management of the labially displaced canine
. J Orthod Res 2015;3:141-5 |
| Introduction | |  |
The prevalence of impacted maxillary canines is 1-2% in the general population. [1],[2] The etiology of impaction is multifactorial. Some of the common causes are genetic predisposition, anomalies in maxillary lateral incisors, and inadequate arch space. [3],[4] Regardless of the cause of the impaction, early treatment to prevent damage to the maxillary lateral incisor is recommended.
The permanent maxillary canine exhibits an eruption pattern slightly buccal to the line of the arch. [5] Because of the path of eruption, the canine will erupt buccally to its natural position in the presence of crowding. [6] Buccally displaced canines have shown a strong correlation with increased arch crowding when compared to palatally displaced canines which are often correlated with excess space in the maxillary arch. [7]
The permanent canines are the foundation of a balanced smile and functional occlusion. [8] Canines also provide a major support for the cheek. Absence of the canine accentuates the appearance of a flattened upper lip. Bowman and Johnston have reported that if a patient's lower lip is 2 or 3 mm behind the E-plane, the profile will worsen after extraction treatment. They also reported that extraction treatment can produce improved facial esthetics for patients who have crowding and protrusion. [9] Extraction patients tend to have an average of 2-4 mm flatter profiles than nonextraction patients at the end of treatment. [10]
Treatment options that are proposed for the treatment of a severely displaced tooth with crowding include extraction or nonextraction. A nonextraction approach may include expansion, interproximal reduction, molar distalization, incisor proclination.
In this case report, we present treatment planning and management of a patient with labially displaced maxillary canine.
| Diagnosis and Etiology | | |
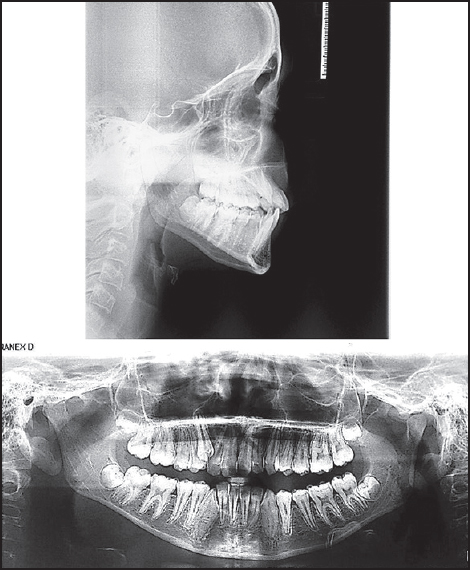
A boy, aged 12 years and 6 months presented with the chief complaint of the buccally erupted ectopic maxillary canine. The patient presented a symmetrical face and a convex profile. When smiling, the patient showed 70% display of maxillary incisors [Figure 1]. Intraoral examination revealed an end on molar and canine relation on the left side and Class I molar relationship on the right side, 3 mm overjet. The maxillary arch exhibited severe constriction, cross bite associated with UL3, UL4, UL5. The maxillary UR3 had erupted ectopically in the arch with minimal attached tissue. There was 5 mm and 1 mm of maxillary midline deviation to the right side and mandibular midline deviation to the left side, respectively. Both the arches showed severe crowding with severely rotated LL3, LR3 [Figure 2]. Cast analysis showed arch length discrepancy of 9 mm in the maxillary arch and 11 mm in the mandible. The panoramic radiograph showed no pathologies. The maxillary and mandibular third molars were developing. The lateral cephalometric analysis revealed the patient had a skeletal Class I relationship (ANB: 1°, Wits: 0 mm) with a normodivergent growth pattern (SN-MP: 34°). The patient's maxillary incisors were (U1-SN: 104°), and the mandibular incisors were uprighted (IMPA: 91°) [Figure 3].
| Treatment Objectives | | |
The treatment objectives were to correct the transverse discrepancy of the maxillary arch, correct ectopic position of the maxillary canine, correct the maxillary midline discrepancy, establish a Class I molar and canine relationship, relieve the crowding in both arches and improve the patient's profile.
| Treatment Plan | | |
On the basis of diagnostic records, a treatment plan was divided into two phases.
Phase I: The treatment plan involved the expansion of the maxillary arch with fixed Quad-Helix until lingual cusp of maxillary premolars and molars touches the buccal cup of mandibular premolars and molars. Before cementation of the Quad-Helix, the desirable force level of 400 g was delivered by activating the appliance by approximately 6-7 mm was done extra orally.
Phase II: Full-size metal maxillary and mandibular fixed appliance to bring the canines into alignment, relieve crowding, to correct midlines.
Long-term retention with canine to canine lingual-bonded retainers on both arches along with Hawley's retainer.
| Treatment Progress | | |
After 4 months of good compliance with the fixed Quad-Helix sufficient amount of expansion was achieved (palatal cusps of the upper molars meet edge-to-edge with the buccal cusps of the mandibular molars) and spacing in the upper arch was present. Full-size metal brackets 0.018-inch MBT preadjusted appliance (American orthodontics) on maxillary, and mandibular arches were bonded. The planned archwire sequence started with 0.012-in NiTI, 0.014-in NiTI, 0.016-in NiTi, 16 NiTi × 22 NiTi for the period of 5 months. Maxillary arch wires were placed in the mandibular arch for the arch coordination and to gain space for the alignment of canine. Later, it was observed there was not enough space in the mandibular arch for the canines to get aligned, proximal stripping of LL4, LL5, LR4, LR5 was performed and alignment was carried out. The wires were changed every 4-5 weeks. Quad-Helix was removed on the 9 th month of the treatment. Five months after the fixed appliance therapy, 16 SS × 22 SS wire was placed in both maxillary and mandibular arches. To maintain the canine space, shift the midline to the left side and prevent any inclination of the adjacent teeth during traction, an open-coil spring was threaded between UR2-UR4 onto the 16 SS × 22 SS main archwire, 0.014 followed by 0.016 temperature-sensitive NiTi as a piggyback wire was fully engaged into it and was ligated on top of the main archwire (16 SS × 22 SS) on the adjacent maxillary lateral incisors and maxillary first bicuspid brackets for the period of 3 months. At the end of the 12 th month UR3 was well aligned into the arch and 16 SS × 22 SS (Streight™ Woven, American orthodontics) in maxillary arch and 16 SS × 22 SS in mandibular arch was placed for the period of 2 months. Final records were made before debonding and final bracket repositioning was done, continuous steel ligation from UR6-UL6, LR6-LL-6, and posterior settling elastics were given for next 2 months followed by 16 SS × 22 SS for last 2 months.
At the end of treatment, the patient had a much-improved esthetic smile, which had been the primary reason for seeking treatment.
The total treatment time was 18 months. Long-term retention with maxillary fixed retainer was bonded to keep the ectopic canine in an optimal position. A mandibular fixed retainer was bonded at the same time along with full-time wear of Hawley's retainer with labial bows canine to canine were given. To ensure continued satisfactory posttreatment alignment of the maxillary and mandibular anterior dentition, the continued use of fixed or removable retainers is recommended indefinitely. [11]
At the end of orthodontic treatment, the patient was referred to his oral surgeon to evaluate his third molars for extraction.
Patient compliance was excellent throughout the treatment.
| Treatment Results | | |
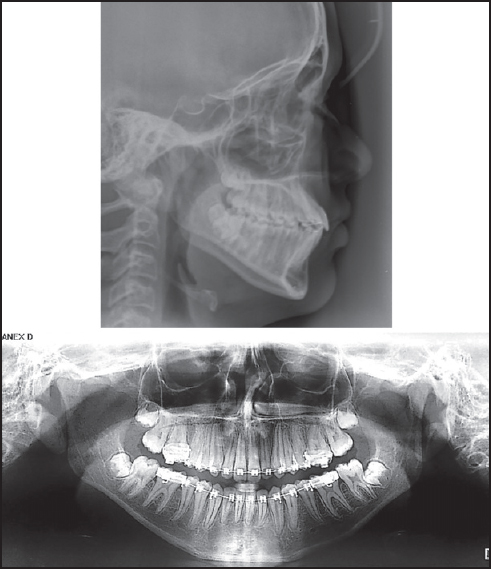
The posttreatment extraoral photographs show general improvement in the facial profile with much-improved aesthetic smile [Figure 4]. Posttreatment intraoral photographs and dental casts show well-expanded dental arches, satisfactory dental alignment, Class I molar and canine relationship on both sides, and normal overjet and overbite. Both maxillary and mandibular midlines are coinciding with a facial midline [Figure 5]. Panoramic radiograph shows good intercuspation, interproximal contacts, and a satisfactory root parallelism and no root resorption were achieved. Posttreatment lateral cephalogram shows no changes in mandibular incisors angulation whereas there was 2° of incisor proclination in the maxillary arch [Figure 6].
| Discussion | | |
Maxillary canines that are potentially impacted or ectopically erupting may be inadvertently overlooked in the mixed dentition patient. This is due to individual variations in eruption patterns and timing. The amount of space in the dental arch for an unerupted canine can be assessed by performing a space analysis. Space for the unerupted canine can be gained by expansion of the maxillary arch, proclination of maxillary incisors or extraction of the permanent premolars.
In the above case reports adequate result was achieved through a nonextraction treatment approach that is, by maxillary expansion using Quad-Helix followed by fixed orthodontic treatment. If four premolars were extracted, it might have resulted in the over retraction of the maxillary anterior teeth with a harmful result to the patient's profile.
McConnell et al. founded an association between maxillary canine impaction and maxillary transverse deficiency. They investigated intermolar width and intercanine width in subjects with impacted maxillary canines and controls without impacted canines. [12] No difference was detected between groups intermolar widths, but the patient with maxillary canine impactions had transverse deficiencies in intercanine arch width compared with controls. They concluded that maxillary orthopedic expansion would be an interceptive modality in treating patients with palatal displaced canines. However, Langberg and Peck concluded that maxillary arch width was not a primary contributory factor in the genesis of the palatal displaced canine. [13] Jacoby also reported that 83% of arches with labial displacement of the maxillary canine displayed arch length deficiency. However, he concluded that arch length deficiency was not associated with palatal displaced canines. [14] Becker et al. reported that tooth size and dental arch dimensions are determining factors in dental crowding, but no reported attempts have so far been made to study the specific reason for the dentoalveolar disproportion (lack of space) found in the majority of subjects with labial displacement of maxillary canine. [15]
Although, the present case could not confirm whether the cause of canine impaction was due to the maxillary transverse discrepancy. After expansion, however, the displaced canine occupied an improved position, and this result facilitated the process of orthodontic forced eruption using a fixed appliance.
The intercanine width in the mandible was increased, but the correction was mostly from uprighting the labial tilted mandibular right canine. To avoid relapse in the future bonded retainers are the retainer of choice. One study showed that long-term changes in incisor alignment are extremely variable and that relapse near 50%, despite occlusion is stable at the time of removing appliance. [16] This would support fixed retention in this case and in many cases where the relapse potential is increased.
| Conclusion | | |
Alignment of ectopically impacted canines is a challenging, but achievable, option. A meticulous biomechanical plan is essential for successful resolution of such a severe malocclusion. Early intervention might be advisable in patients with impacted canines as a cautious measure, preventing possibly greater complexity of the orthodontic treatment from altered paths of eruption. Patients with a transverse discrepancy are more likely to have an impacted canine than are patients without a transverse discrepancy. Correct treatment planning combined with space management and properly directed light continuous traction force are the three main factors to determine the success of every impacted case. The decision to expand the arches is to be good esthetically, functionally, and for more stable results in these patients. In the light of the attention currently being paid to esthetics as a primary treatment goal for both practitioner and patient, today's treatment plans for patients with ectopic canine must consider more than the orthodontic outcome.
| References | | |
| 1. | Bass TB. Observations on the misplaced upper canine tooth. Dent Pract Dent Rec 1967;18:25-33.  |
| 2. | Rayne J. The unerupted maxillary canine. Dent Pract Dent Rec 1969;19:194-204. |
| 3. | Vastardis H. The genetics of human tooth agenesis: New discoveries for understanding dental anomalies. Am J Orthod Dentofacial Orthop 2000;117:650-6. |
| 4. | Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod 1994;64:249-56. |
| 5. | Basdra EK, Kiokpasoglou MN, Komposch G. Congenital tooth anomalies and malocclusions: A genetic link? Eur J Orthod 2001;23:145-51. |
| 6. | Bedoya MM, Park JH. A review of the diagnosis and management of impacted maxillary canines. J Am Dent Assoc 2009;140:1485-93. |
| 7. | Jacoby H. The etiology of maxillary canine impaction. Am J Orthod 1982;84:125-89. |
| 8. | Richardson G, Russell KA. A review of impacted permanent maxillary cuspids - Diagnosis and prevention. J Can Dent Assoc 2000;66:497-501. |
| 9. | Bowman SJ, Johnston LE Jr. The esthetic impact of extraction and nonextraction treatments on Caucasian patients. Angle Orthod 2000;70:3-10. |
| 10. | Stephens CK, Boley JC, Behrents RG, Alexander RG, Buschang PH. Long-term profile changes in extraction and nonextraction patients. Am J Orthod Dentofacial Orthop 2005;128:450-7. |
| 11. | Little RM, Riedel RA, Artun J. An evaluation of changes in mandibular anterior alignment from 10 to 20 years postretention. Am J Orthod Dentofacial Orthop 1988;93:423-8. |
| 12. | McConnell TL, Hoffman DL, Forbes DP, Janzen EK, Weintraub NH. Maxillary canine impaction in patients with transverse maxillary deficiency. ASDC J Dent Child 1996;63:190-5. |
| 13. | Langberg BJ, Peck S. Adequacy of maxillary dental arch width in patients with palatally displaced canines. Am J Orthod Dentofacial Orthop 2000;118:220-3. |
| 14. | Jacoby H. The etiology of maxillary canine impactions. Am J Orthod 1983;84:125-32. |
| 15. | Becker A, Sharabi S, Chaushu S. Maxillary tooth size variation in dentitions with palatal canine displacement. Eur J Orthod 2002;24:313-8. |
| 16. | Artun J, Garol JD, Little RM. Long-term stability of mandibular incisors following successful treatment of Class II, Division 1, malocclusions. Angle Orthod 1996;66:229-38. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6]
|














 Search Pubmed for
Search Pubmed for