|
 
 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 2
| Issue : 3 | Page : 162-167 |
|
Simultaneous retraction and intrusion using a single palatal micro-implant
Ketan K Vakil, Murlidhar R Sastri, Jeegar K Vakil
Department of Orthodontics and Dentofacial Orthopedics, SMBT Dental College, Ghulewadi, Sangamner, Maharashtra, India
| Date of Web Publication | 12-Sep-2014 |
Correspondence Address:
Ketan K Vakil
Department of Orthodontics and Dentofacial Orthopedics, SMBT Dental College, Ghulewadi, Sangamner - 411 008, Maharashtra
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.140689

This case report describes the treatment of a case with skeletal Class II, gummy smile, anterior deep bite and convex facial profile. While treating such a severe case, the outcome may not always be successful with orthodontic therapy alone. For this reason, surgical therapy is often chosen to gain an esthetic facial profile and a good smile. However, sometimes the patients reject surgical treatment and an alternative method must be considered. Skeletal anchorage systems such as miniscrews are now frequently used for correcting severe malocclusion that should be treated by orthodontics and surgical therapy. In this case report, we treated a skeletal Class II malocclusion with convex profile and gummy smile using miniscrews, which were placed in the mid-palatal region for simultaneous intrusion and retraction of upper anteriors. Keywords: Class II correction, gummy smile, miniscrew
How to cite this article:
Vakil KK, Sastri MR, Vakil JK. Simultaneous retraction and intrusion using a single palatal micro-implant. J Orthod Res 2014;2:162-7 |
| Introduction | |  |
The use of skeletal anchorage systems has become a new orthodontic treatment strategy over the past decade. [1],[2],[3],[4],[5],[6],[7],[8],[9] Miniscrews, as an alternative method for absolute anchorage have been extensively used. The major advantages compared with dental implants or microplates are small size, allowing placement in many intra-oral areas, low cost, and easy implantation and removal.
Various sites have been proposed for the placement of miniscrews, one of them being the mid-palatal region. The advantages of placing the miniscrews in the mid-palatal region are good primary stability, do not limit the amount of distalization and the line of application of force can be altered as per the desired tooth movement.
Distalization of maxillary molars has been tried and tested with various extra-oral and intra-oral appliances with varying degree of success and disadvantages of the maxillary molar extrusion and proclination of anteriors. In contrast, the miniscrews provide sufficient anchorage for incisor retraction in Class II treatment without unwanted orthodontic side effects.
Gummy smile is an esthetic problem for patients and a frequent finding that can occur as a result of various intra-oral or extra-oral etiologies. [10],[11],[12],[13],[14] Thus, proper diagnosis and treatment are important. If a gummy smile is characterized by overgrowth of anterior vertical maxillary excess, the outcome may not always be successful with conventional orthodontic therapy alone. In such cases, surgical therapy, such as that provided by a Le Fort impaction or maxillary gingivectomies, are often chosen to gain a good smile.
However, if the patients are unwilling to undergo surgical treatment, an alternative method must be considered to treat the gummy smile. Miniplates and miniscrews [15],[16],[17] are now frequently used for establishing absolute anchorage for orthodontic tooth movement.
In this case report, we present the management of a skeletal Class II patient with the gummy smile, prominent premaxilla and convex facial profile using palatal micro-implant.
| Case Report | | |
A female patient (P.C) aged 12-year-old visited the department with the chief complaint of irregular and forwardly placed upper front teeth with excessive gingival display. Extra-oral examination revealed convex facial profile. Frontal view at rest showed prominent premaxillary segment and vertical maxillary excess. There was an increased maxillary incisor display and gummy smile [Figure 1].
Dentally, there was crowding in the upper arch with a retained upper right deciduous canine and upper right canine was erupting labially, bilateral Class II molar relation, anterior deep bite and an increased overjet and maxillary midline was shifted to the left. Oral hygiene condition was fair [Figure 2]. Soft tissue examination revealed an acute nasolabial angle and incompetent lips.
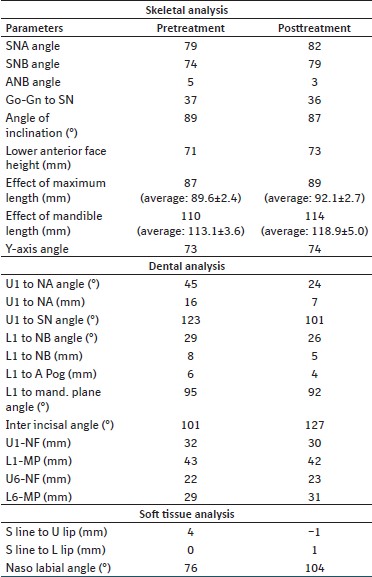
The cephalometric examination [Table 1] showed skeletal Class II relation due to prognathic maxilla and orthognathic mandible. Maxilla also showed an increase in the vertical plane [Figure 3]. | Figure 3: (a) Pretreatment cephalogram and (b) pretreatment orthopantomogram
Click here to view |
Treatment Objectives
- Correction of anterior deep bite and "gummy" smile.
- Correction of overjet.
- Correction of crowding in the upper arch.
- Establishing Class I molar, canine and incisor relationship.
- Improving the overall facial esthetics.
Treatment Plan
- Extraction of over-retained upper right deciduous canine.
- Fixed mechanotherapy using preadjusted edgewise appliance (0.018 MBT).
- Placement of palatal micro-implant for simultaneous intrusion and retraction of maxillary teeth.
- Finishing and detailing followed by retention.
Treatment Progress
Following extraction of over-retained upper right deciduous canine, preadjusted edgewise fixed appliances (0.018" slot, MBT prescription) were placed in the upper and lower dentition. The arches were leveled and aligned with upper and lower 0.014 HANT archwires. As the lower arch was minimally crowded, leveling, and alignment was achieved in 6 weeks. Upper right canine was brought into alignment in about 8 weeks. 0.016 × 0.022 nickel titanium (NiTi) archwires were placed in upper and lower arches for better leveling and alignment for 4 weeks. This was followed by 0.016 Australian stainless steel archwire in the upper arch to consolidate spaces. Upper and lower co-ordinated 0.016 × 0.022 stainless steel were then placed.
Placement of micro-implant (Dentos, 1615-08) was done in the mid-palate under thorough aseptic conditions using surface anesthetic gel (benzocaine 5% - ultradent products). Contra-angled hand-driver (Dentos, India) was used for placement of micro-implant in the mid-palatal region [Figure 4]. The angulation of the contra-angled hand-driver allowed better accessibility to facilitate micro-implant placement perpendicular to the palatal surface [Figure 5] and [Figure 6]. NiTi closed coil spring (12 mm) was used for simultaneous intrusion and retraction of the maxillary dentition. One end of the coil spring was ligated to the head of micro-implant while the other end was stretched and ligated between the central incisors labially. Force of about 300-350 g was used. Proper oral hygiene instructions were emphasized to prevent any gingival inflammation due to coil spring. Force application being oblique and passing through or above the center of rotation of maxillary dentition, it enabled rotation of the occlusal plane anteriorly upwards [Figure 7]. Simultaneous intrusion and retraction of maxillary dentition was achieved in about 14 months, which was followed by 0.017 × 0.025 co-ordinated stainless steel archwires in upper and lower arches. Class II elastics were then placed for a period of 6 weeks. Finishing and detailing of the case was done along with minor settling of the posterior occlusion. Direct bonded retainers were placed in the upper and lower arches, which were supplemented with Hawley's retainers on debonding. | Figure 4: Armamentarium for placement of palatal micro-implant. (a) Contra-angle driver, (b) contra-angle handpiece, (c) hand-driver
Click here to view |
 | Figure 5: As per Figure 4 Parts a– c - assembled together prior to micro-implant placement
Click here to view |
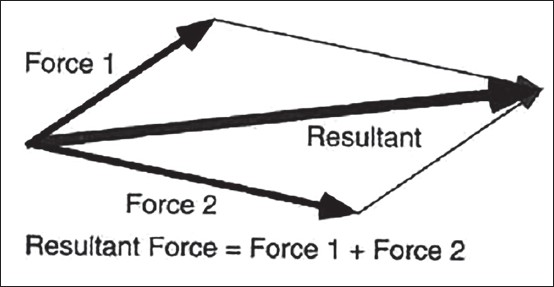 | Figure 7: Resultant line indicating the line of force using palatal implant for simultaneous intrusion and retraction in relation to the occlusal plane
Click here to view |
Active treatment time was about 20 months. The retention phase is in progress.
Treatment Results
A normal overjet and overbite were achieved and the upper and lower midlines coincided. The upper and lower dental arches were well-aligned, and a Class I molar relationship was achieved [Figure 8]. The strain of the mentalis muscle reduced. The facial profile was significantly improved [Figure 9]. The posttreatment panoramic radiograph showed that the all the roots were parallel and root resorption was not observed [Figure 10]. Gingival exposure post treatment was dramatically reduced as a result of intrusion of the anterior teeth [Figure 11],[Figure 12] and [Figure 13], and the patient obtained a good smile.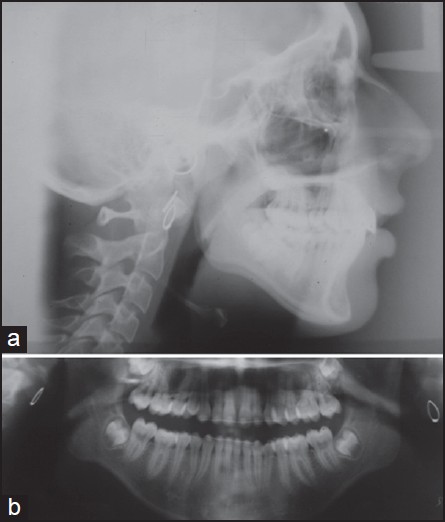 | Figure 10: (a) Posttreatment cephalogram and (b) posttreatment orthopantomogram
Click here to view |
1 year Post-treatment results are shown in [Figure 14] and [Figure 15] respectively.
| Discussion | | |
Excessive gingival display can be divided into several categories according to etiologic factors (e.g., downward growth of maxilla, short upper lip, and hypertropic gingiva). Dentoalveolar excessive gingival display occurs due to overgrowth of the maxillary anterior dentoalveolar height. It is difficult to intrude anterior section with normal orthodontic mechanotherapy like J-hook headgear or utility arch. For this reason, surgical impaction of the maxillary anterior dentoalveolar region is often applied in severe gummy smile cases.
Moreover, since impaction of the anterior segment by Le Fort I tend to increase nasal alar width, which could make the patient's nose wider. Thus, we have to decide carefully whether to apply surgical or nonsurgical treatment modality.
On the other hand, implants for orthodontic anchorage, such as miniplates and miniscrews, have recently been developed. Miniscrews can be placed bucally or palatally to achieve desired treatment results.
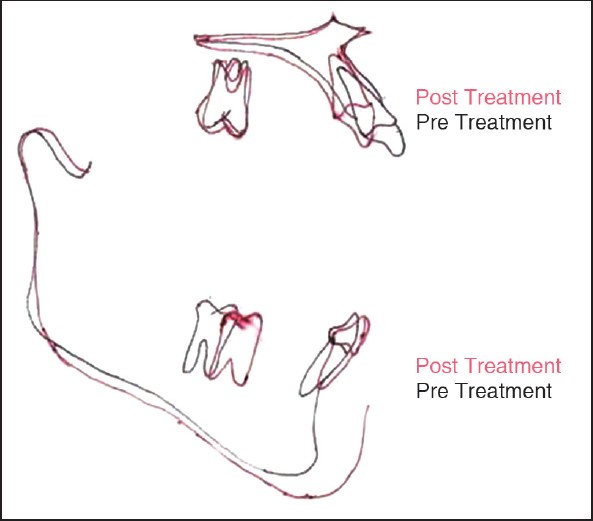
The patient in this case report had dentoalveolar gummy smile and the posterior teeth were in normal vertical positions. In this category, gummy smile can be corrected efficiently by intrusion and retraction of maxillary incisors. Therefore, we planned to intrude the upper incisors with miniscrews, which could provide a desirable improvement of the smile. In general, miniscrews for intrusion of incisors are placed between the roots of the anterior teeth. In this case, we inserted the miniscrew in the mid-palatal region between the maxillary first molars and applied the distal driving force with the help of NiTi coil spring. This vector of force delivered simultaneous retractive and intrusive force to the anterior segment. This effectively brought about a drastic change in the patients profile and smile.
| Conclusions | | |
- Severe gummy smile can be treated with miniscrews through intrusion of the upper incisors.
- The patient's profile can be improved by correction of overjet using miniscrews.
- Simultaneous retraction and intrusion of maxillary anteriors can be achieved by proper placement of mini screw and proper application of force.
| References | | |
| 1. | Roberts WE, Helm FR, Marshall KJ, Gongloff RK. Rigid endosseous implants for orthodontic and orthopedic anchorage. Angle Orthod 1989;59:247-56. 
|
| 2. | Umemori M, Sugawara J, Mitani H, Nagasaka H, Kawamura H. Skeletal anchorage system for open-bite correction. Am J Orthod Dentofacial Orthop 1999;115:166-74.
|
| 3. | Creekmore TD, Eklund MK. The possibility of skeletal anchorage. J Clin Orthod 1983;17:266-9.
[PUBMED] |
| 4. | Kuroda S, Katayama A, Takano-Yamamoto T. Severe anterior open-bite case treated using titanium screw anchorage. Angle Orthod 2004;74:558-67.
|
| 5. | Kuroda S, Sugawara Y, Yamashita K, Mano T, Takano-Yamamoto T. Skeletal Class III oligodontia patient treated with titanium screw anchorage and orthognathic surgery. Am J Orthod Dentofacial Orthop 2005;127:730-8.
|
| 6. | Kyung HM1, Park HS, Bae SM, Sung JH, Kim IB. Development of orthodontic micro-implants for intraoral anchorage. J Clin Orthod 2003;37:321-8.
[PUBMED] |
| 7. | Kuroda S, Sugawara Y, Deguchi T, Kyung HM, Takano-Yamamoto T. Clinical use of miniscrew implants as orthodontic anchorage: Success rates and postoperative discomfort. Am J Orthod Dentofacial Orthop 2007;131:9-15.
|
| 8. | Park HS, Lee SK, Kwon OW. Group distal movement of teeth using microscrew implant anchorage. Angle Orthod 2005;75:602-9.
|
| 9. | Park HS, Kwon TG, Sung JH. Nonextraction treatment with microscrew implants. Angle Orthod 2004;74:539-49.
|
| 10. | Peck S, Peck L, Kataja M. Some vertical lineaments of lip position. Am J Orthod Dentofacial Orthop 1992;101:519-24.
|
| 11. | Hunt O, Johnston C, Hepper P, Burden D, Stevenson M. The influence of maxillary gingival exposure on dental attractiveness ratings. Eur J Orthod 2002;24:199-204.
|
| 12. | Garber DA, Salama MA. The aesthetic smile: Diagnosis and treatment. Periodontol 2000 1996;11:18-28.
|
| 13. | Redlich M, Mazor Z, Brezniak N. Severe high Angle Class II Division 1 malocclusion with vertical maxillary excess and gummy smile: A case report. Am J Orthod Dentofacial Orthop 1999;116:317-20.
|
| 14. | Polo M. Botulinum toxin type A in the treatment of excessive gingival display. Am J Orthod Dentofacial Orthop 2005;127:214-8.
[PUBMED] |
| 15. | Kanomi R. Mini-implant for orthodontic anchorage. J Clin Orthod 1997;31:763-7.
[PUBMED] |
| 16. | Park HS, Bae SM, Kyung HM, Sung JH. Micro-implant anchorage for treatment of skeletal Class I bialveolar protrusion. J Clin Orthod 2001;35:417-22.
|
| 17. | Paik CH, Woo YJ, Boyd RL. Treatment of an adult patient with vertical maxillary excess using miniscrew fixation. J Clin Orthod 2003;37:423-8.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9], [Figure 10], [Figure 11], [Figure 12], [Figure 13], [Figure 14], [Figure 15]
[Table 1]
|



















 Search Pubmed for
Search Pubmed for