|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 2
| Issue : 3 | Page : 149-155 |
|
The effect of functional orthopedic treatment with removable appliance on young adults
Ahmad Abdallah Rahhal
Department of Orthodontics, Faculty of Dentistry, Arab American University-Jenin, West-Bank, Palestine
| Date of Web Publication | 12-Sep-2014 |
Correspondence Address:
Ahmad Abdallah Rahhal
Department of Orthodontics, Faculty of Dentistry, Arab American University-Jenin, West-Bank
Palestine
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.140686

Objective: To evaluate the treatment effects of a removable functional appliance (modified bionator) on young adults. Materials and Methods: A total of 12 skeletal CLII (class two) female patients, with average skeletal age 15.8-years old, used the modified bionator 16 h a day for 8 months. Lateral cephalometric X-rays were taken and analyzed before and after the treatment using paired t-test. Hand wrist X-rays were taken before the application of the appliance only. Results: After 8 months of treatment Angle CLI (class one) relationship was achieved; there was a significant reduction in the ANB (A-point Nasion B-point), SNA (Sella-Nasion-Apoint), face convexity, and overjet. SNB (Sella-Nasion-Bpoint) and face length significantly increased. Conclusion: The removable functional appliance - modified bionator - is an available option for correcting of borderline skeletal class II malocclusion in young adults or patients in late developmental stage. Keywords: Functional treatment, modified bionator, young adults
How to cite this article:
Rahhal AA. The effect of functional orthopedic treatment with removable appliance on young adults. J Orthod Res 2014;2:149-55 |
| Introduction | |  |
Among all malocclusions, CLII contributes approximately 15%. The CLII malocclusion is used to describe the condition in which the mandibular first molars occlude distal to the normal relationship with the maxillary first molars. CLII can be further divided to dental and skeletal malocclusions. [1] Two treatment options are available for young adult patients with skeletal class II malocclusion caused by mandibular deficiency. The first option is combined surgical and orthodontic treatment, which lengthens the mandible anteriorly through mandibular sagittal split osteotomy; this, in turn, can correct the skeletal and soft tissue relationship. [2],[3],[4] The second option is functional orthopedic treatment, Herbst appliance therapy, which reactivates condylar growth to correct mandibular deficiency. [5],[6],[7],[8],[9],[10],[11] In consecutively treated class II division 1 malocclusion cases, the immediate as well as the short-term follow-up effects of the Herbst appliance [12] have been thoroughly analyzed in several investigations. [13],[14],[15],[16],[17],[18],[19],[20]
At the end of functional treatment, an overcorrected class I dental arch relationship with incomplete cuspal interdigitation is a common finding. [21],[22],[23],[24] In general, after the first 6 months of functional treatment, however, the occlusion settles into class I due to recovering tooth movements. [25],[26]
When relating the appliance effects to the patient's level of somatic maturation at therapy, a larger increase in sagittal condylar growth was found when treatment was performed at peak height velocity of growth than when treatment was performed before or after that period. [15],[27]
Previous researchers looked into the possibility of stimulating growth of the condyle in adults. Among them, Xiong et al., [21],[22],[23],[24] showed that forward mandibular positioning affected the biophysical environment of the temporomandibular joint (TMJ), and this induced recruitment of mesenchymal cells. These cells underwent endochondral ossification, which resulted in new bone formation in adult rats. Purkayastha et al., [11] demonstrated the formation of new cartilage and bone in the condylar areas of adult patients, along with a concomitant reduction in facial convexity, following stepwise Herbst appliance therapy. The studies mentioned earlier suggest that there exists a possible nonsurgical treatment modality for skeletal class II malocclusion in adults, especially among borderline cases.
The previous studies that evaluated the effects of the functional treatment on young adults usually used fixed functional appliances like Herbst and forsus. [10],[28],[29]
The aim of this research was to evaluate the treatment effects of a removable functional appliance (modified activator) on young adults.
| Materials and Methods | | |
The patient group consisted of 12 females and four males, exhibiting skeletal and dental CLII due to mandibular retrognathism [Figure 1]. The four males were excluded from the research because of low cooperation. The chronological age was 15.5 years (14.5-16) and the skeletal age was 15.8 years (14.5-16.5). The growth potential of the patients was 0.9% (0.3-1.4%). The skeletal age was predicted using hand wrist X-rays, which were taken in the beginning of the treatment. All patients were in the stages between MP3 union and Ru stages according to the hand-wrist Atlas More Details. [30] | Figure 1: One of the patients profi le photos, before and after the treatment
Click here to view |
Patient Selection Criteria
The patients were selected from the clinic of the Arab American University. The patient selection criteria included the following:
- Skeletal and dental CLII due to mandibular retrognathism
- Late stage of growth and development (less than 1.5% of growth potential).
- All patients were in the stages between MP3 union and Ru stages.
Appliance Design
The original bionator appliance was modified by replacing the palatal and lingual arches with acrylic to acquire maximum skeletal pressure on the mandibular lingual bone and maximum anchorage from the palatal side [Figure 2] and [Figure 3]. All the patients were asked to use the appliance 16 h a day for 8 months. We believed that after 8 months, the residuals of the growth and development will be completely ceased. To ensure the treatment results, the patients used the appliance for another 6 moths at night for retention. | Figure 3: Extraoral photograph of the modified bionator, the lingual and palatal arches were replaced by acrylic
Click here to view |
Cephalometric Analysis
To predict the results of the treatment, lateral cephalometric X-rays were taken before and after the treatment. All cephalograms were traced manually on acetate paper by the same doctor. Cephalometric planes for dental, skeletal, and soft tissue measurements are illustrated in [Figure 4],[Figure 5],[Figure 6] and [Figure 7].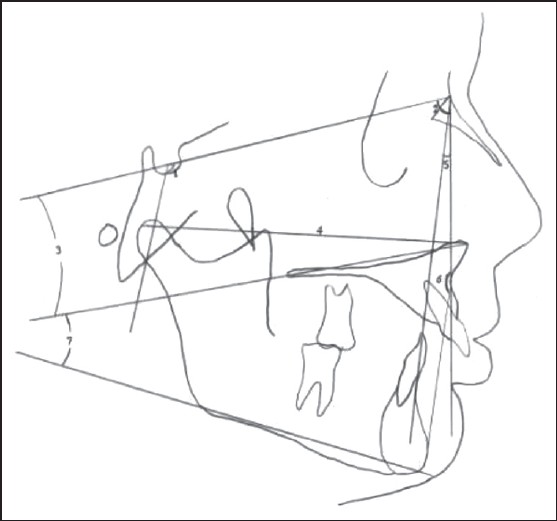 | Figure 4: Cranial, maxillar, and maxillomandibular values used in the research. Cranial: 1-N-S-Ar (Eyer angle). Maxillar: 2-SNA angle, 3-SN/ANS-PNS (palatal plane to SN angle), 4-Co-ANS length. Maxillomandibular: 5-ANB angle, 6-N-A-Pg angle, 7-ANS-PNS/Go-Gn maxillomandibular angle
Click here to view |
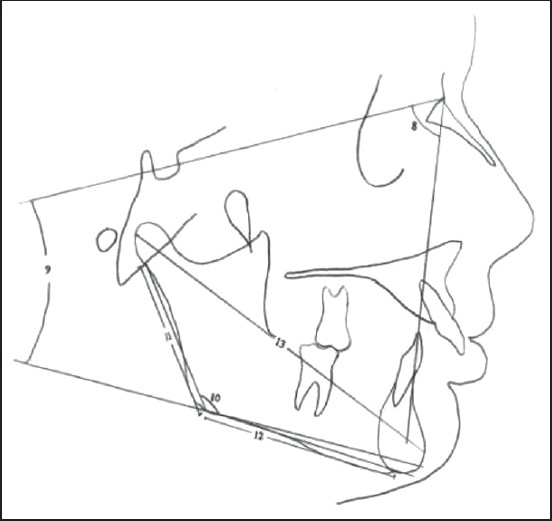 | Figure 5: Mandibular measurements used in the research. 8-SNB angle, 9-SN/Go-Gn angle, 10-Ar-Go-M articular angle, 11-Ar-Go ramus length, 12-Go-M corpus length, 13-Co-Pg effective mandibular length
Click here to view |
 | Figure 6: Face-height, dental and dentoalveolar measurements used in the research. 14-N-ANS upper face height, 15-ANS-M lower face height, 16-N-M anterior total face height, 17-S-Go posterior face length, 18-over-jet, 19-overbite, 20-U6⊥ANS-PNS upper posterior dentoalveolar height, 21-U1⊥ANS-PNS upper anterior dentoalveolar height, 22-L6⊥Go-M lower posterior dentoalveolar height, 23-L1⊥Go-M lower anterior dentoalveolar height, 24-U6⊥Ptv upper fi rst molar to pterogoid vertical length, 25-L6⊥Ptv lower fi rst molar to pterogoid vertical length, 26-U1⊥Ptv upper incisor to pterogoid vertical length, 27-L1⊥Ptv lower incisor to pterogoid vertical length, 28-U1/SN angle, 29-L1/Go-Gn angle, 30-U1/L1 interincisal angle
Click here to view |
 | Figure 7: Soft tissue measurements. 1. upper lip thickness, 2. Lower lip thickness, 3. Lab. sup. ⊥RL, 4. Lab. inf. ⊥RL, 5. Pg_ ⊥RL, 6. H-angle, 7. E-line upper lip, 8. S-line upper lip, 9. E-line lower lip, 10. S-line lower lip
Click here to view |
Statistical Method
The data obtained from the cephalometric tracings were evaluated statistically by using the t-test, Statistical Package for the Social Sciences (SPSS) version 17 was used. Operator precision was tested by random selection of seven of the cephalograms before and after treatment. The tracings and measurements were repeated 3 weeks after the first measurements. Correlation analysis applied to the same measurements showed the high ranges for r values (0.096-1.00).
No control group from same age was used for ethical reasons. It is not ethical to use individuals from the same skeletal age and miss the chance of treating them without surgery.
| Results | | |
During the treatment, the cooperation of the patients was very good. Full Angle CLI relationship was achieved after 6 months, and the posttreatment cephalometrics were taken after 8 months of the appliance usage to be sure of the end of the growth and development. The results of the cephalometric X-ray tracing are shown in [Table 1] and [Table 2]. | Table 1: The results of the paired t-test of the skeletal and dental variables before and after the treatment
Click here to view |
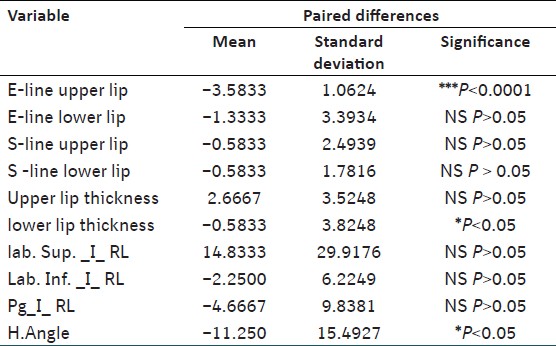 | Table 2: The results of the paired t-test of the soft tissue variables before and after the treatment
Click here to view |
Skeletal Changes
SNA decreased significantly (−1.000°, P < 0.001); ANB showed significant decrease (−2.333, P < 0.0001), whereas B point moved forward (2.333 mm, P < 0.0001) Co-Pg length increased significantly (4.167 mm, P < 0.0001), N-ANS, ANS-Me significantly increased causing a significant increase in the total face height N-Me (3.000 mm, P < 0.0001), S-Go distance showed significant increase (2.500 mm, P < 0.0001).
Dent Alveolar Changes
The upper incisor teeth were retroclined and the lower incisor teeth were proclined significantly resulting in a very significant decrease in the over jet (7.333 mm, P < 0.0001), Ptv_U1 (5.333 mm, P < 0.001), and SN_U1 (15.000°, P < 0.0001). Ptv_U6 showed significant decrease (1.667 mm, P < 0.001). The upper and lower incisor teeth were extruded significantly ANS-PNS_U1 (1.833 mm, P < 0.0001). The lower molar teeth significantly drifted mesialy Ptv_L6 (3.250 mm, P < 0.001). The interincisal angle UI_L1 showed significant increase (14.333 degree, P < 0.0001).
Soft Tissue Changes
The soft tissue variables in general did not change significantly after treatment, except for the upper lip that has retruded significantly after treatment upper lip E-Line (-3.5833 mm, P < 0.0001), the lower lip thickness decreased significantly (−0.5833 mm, P < 0.05), and also the H-angle decreased significantly (−11.250°, P < 0.05).
| Discussion | | |
Very few studies examined the effect of the functional orthopedic treatment on young adults and individuals in the very late stage of growth and development. All these studies searched the effect of the fixed functional appliances, [10],[28],[29] thus the aim of this research was to examine the effect and the efficiency of a removable functional appliance on these patients. The original bionator appliance was modified by replacing the lingual and palatal arches with acrylic to maximize the forward pressure on the lingual side of the mandibular bone and the anchorage from the palatal side. This study consisted only female patients. The reason for this might be associated with the fact that women generally showed a greater interest in improving their dental and facial appearance. [25]
Skeletal Findings
The backward movement of the A-point indicates that the appliance has restriction effect on the maxilla, what is known as head gear-like effect of the functional appliances. On the other hand, the B-point moved forward 1.3° due to the growth stimulation of the mandible by the functional appliances. These results are supported by many clinical studies. [28],[29]
The value of the ANB angle showed a statistically significant change after the treatment, it has decreased by about 2.33°. This consisted of both growth restriction of the maxilla and growth stimulation of the mandible. This value is near to the values found by Chaiyongsirisern A, et al., [28] and Adusumilli et al., [29] but it a little far away from the results of Hansen et al., [8] who showed this value as 1.6°. This difference could be distributed to the sex of the patients, our group consisted of females only, whereas the Hansen et al., [8] group consisted of males.
In this study, the effective mandibular length, represented by the Co-Pg distance, increased significantly after treatment. The pogonion might have moved forward as a result of the mandibular length increase or mesial relocation of the mandible as a whole. [31] The situation may be the result of the remodeling processes in the articular fossa. [32],[33],[34],[35],[36]
After the treatment face convexity decreased due to the backward movement of the A-point and the forward movement of the Pg, this was expressed by the significant increase in the N-A-Pg value. This result is similar to many other previous studies. [28],[29],[37]
The downward forward growth of the mandible resulted in an elongation of the anterior face height. [28],[29],[37]
Dental Findings
The significant decrease in the overjet, 7.33 mm, was a combination of skeletal and dental effects, the restriction of the maxillary growth, the enhancement of the mandibular growth, retroclination of the maxillary incisors, and the protrusion of the mandibular incisors. Our finding is similar to the result of studies of Ruf et al., [9] 7.7 mm, and Chaiyongsirisern et al., [28] 8.3 mm, and also it is supported by many previous studies. [8],[11],[29]
There was a significant mesial drift in the lower dental arch PtV_L6 (3.2 mm), PtV_L1 (1.6 mm), and a very significant distal drift in the upper dental arch PtV_U6 (1.6 mm), PtV_U1 (5.4 mm). The protraction amount of the lower incisors is very similar to the results of Kucukkeles et al., [36] but it is small compared with other studies by Ruf et al., [10] and Chaiyongsirisern et al. [28] The reason for that could be the effect of the lower vestibular arch, which prevented the extra protrusion of the lower teeth.
The nonsignificant change in the overbite 1.67 mm, although there was a significant increase in the anterior face height and the effective length of the mandible, was due the significant retraction of the upper incisor teeth and the nonsignificant protraction of the lower teeth.
Soft Tissue Findings
The upper lip moved posteriorly 3.58 mm due to the refraction and retroclination in the upper incisor teeth. This result is supported by Chaiyongsirisern et al. [28] On the other hand, the lower lip did not move forward, which is not supported by other studies [28],[37] due to the minimal protraction of the lower incisor teeth.
The forward movement of the mandible and the Pg resulted in a significant decrease in the soft tissue convexity in the H-angle. This result is supported by Kucukkeles et al.[36]
| Conclusion | | |
The removable functional appliance - modified bionator - is an available option for correcting borderline skeletal class II malocclusion in young adults or patients in late developmental stage.
| References | | |
| 1. | Proffit WR, Fields HW, Sarver DM. Contemporary Orthodontics. Penny Rudolph, 3 rd ed. St Louis: Eldsevier Mosbey; 2007. p. 495-6. 
|
| 2. | Obwegeser HL. The indication for surgical correction of mandibular by sagittal splitting technique. Br J Oral Surg 1964;1:157-71.
|
| 3. | Dal Pont G. Retromolar osteotomy for the correction of prognathism. J Oral Surg Anesth Hosp Dent Serv 1961;19:42-7.
[PUBMED] |
| 4. | Schendel SA, Epker BN. Result after mandibular advancement surgery: An analysis of 87 cases. J Oral Surg 1980;38:265-82.
[PUBMED] |
| 5. | Ruf S, Pancherz H. Orthognathic surgery and dentofacial orthopedics in adult Class II Division 1 treatment: Mandibular sagittal split osteotomy versus Herbst appliance. Am J Orthod Dentofacial Orthop 2004;126:140-52.
|
| 6. | Pancherz H, Ruf S. The Herbst appliance: Research-based updated clinical possibilities. World J Orthod 2000;1:17-31.
|
| 7. | Pancherz H. Dentofacial orthopedics or orthognathic surgery: Is it a matter of age? Am J Orthod Dentofacial Orthop 2000;117:571-4.
[PUBMED] |
| 8. | Hansen K, Pancherz H, Hagg U. Long-term effects of the Herbst appliance in relation to the treatment growth period: Cephalometric study. Eur J Orthod 1991;13:471-81.
|
| 9. | Ruf S, Pancherz H. Temporomandibular joint remodeling in adolescents and young adults during Herbst treatment: A prospective longitudinal magnetic resonance imaging and cephalometric radiographic investigation. Am J Orthod Dentofacial Orthop 1999;115:607-18.
|
| 10. | Ruf S, Pancherz H. Dentoskeletal effects and facial profile changes in young adults treated with the Herbst appliance. Angle Orthod 1999;69:239-46.
|
| 11. | Purkayastha S, Rabie AB, Wong R. Treatment of skeletal Class II malocclusion in adults: Stepwise vs single-step advancement with the Herbst appliance. World J Orthod 2008;9:233-43.
|
| 12. | Herbst E. Dreissighjahrige experience with the retention Hinge. Zahnaerztliche Rundscha 1975; 43:1515-24, 1563-8, 1611-6.
|
| 13. | Pancherz H. Treatment of Class II malocclusions by jumping the bite with the Herbst appliance. A cephalometric investigation. Am J Orthod 1979;76:423-42.
[PUBMED] |
| 14. | Pancherz H. The effect of continuous bite-jumping on the dentofacial complex: A follow-up study after Herbst appliance treatment of Class II malocclusions. Eur J Orthod 1981;3:49-60.
[PUBMED] |
| 15. | Pancherz H. The mechanism of Class II correction in Herbst appliance treatment. A cephalometric investigation. Am J Orthod 1982;82:104-13.
[PUBMED] |
| 16. | Pancherz H. The Herbst appliance - Its biologic effects and clinical use. Am J Orthod 1985;87:1-20.
[PUBMED] |
| 17. | Pancherz H, Fackel U. The skeletofacial growth "pattern pre-and post-dentofacial orthopaedics. A long-term study of Class II malocclusions treated with the Herbst appliance. Eur J Orthod 1990;12:209-18.
|
| 18. | Pancherz H, Hagg U. Dentofacial orthopedics in relation to somatic maturation. An analysis of 70 consecutive cases treated with the Herbst appliance. Am J Orthod 1985;88:273-87.
|
| 19. | Pancherz H, Hansen K. Occlusal changes during and after Herbst treatment: A cephalometric investigation. Eur J Orthod 1986;8:215-28.
[PUBMED] |
| 20. | Pancherz H, Hansen K. Mandibular anchorage in Herbst treatment. Eur J Orthod 1988;10:149-64.
[PUBMED] |
| 21. | Xiong H, Hagg U, Tang GH, Rabie AB, Robinson W. The effect of continuous bite-jumping in adult rats: A morphological study. Angle Orthod 2004;74:86-92.
|
| 22. | Xiong H, Rabie AB, Hagg U. Mechanical strain leads to condylar growth in adult rats. Front Biosci 2005;10:67-73.
|
| 23. | Xiong H, Rabie AB, Hagg U. Neovascularization and mandibular condylar bone remodeling in adult rats under mechanical strain. Front Biosci 2005;10:74-82.
|
| 24. | Rabie AB, Xiong H, Hagg U. Forward mandibular positioning enhances condylar adaptation in adult rats. Eur J Orthod 2006;26:353-8.
|
| 25. | Hoppenreijs TJ, Hakman EC, Vant Hof MA, Stoelinga PJ, Tuinizing DB, Freihofer HP. Psychologic implication of surgical orthodontic treatment in patients with anterior open bite. Int J Adult Orthod Orthognath Surg 1999;14:101-12.
|
| 26. | Eggensperger N, Smolka W, Rahal A, Iizuka T. Skeletal relapse after mandibular advancement and setback in single jaw surgery. J Oral Maxillofac Surg 2004;62:1486-96.
|
| 27. | Dahlberg G. Statistical Methods for Medical and Biological Students. New York: InterScience Publications 1940; p: 25-6.
|
| 28. | Chaiyongsirisern A, Bakr RA, Ricky W, Wong K. Stepwise advancement herbst appliance versus mandibular sagittal split osteotomy treatment effects and long-term stability of adult class II patients. Angle Orthod 2009;79:1084-94.
|
| 29. | Adusumilli SP, Sudhakar P, Mummidi B, Varma DP, Arora S, Radhika A, et al. Biomechanical and clinical consideration in correction CLII malocclusions with Forsus. J Contemp Dent Pract 2012;13:918-24.
|
| 30. | Greulich W, Phyle S. Radiographic Atlas of Skeletal Development of the Hand and Wrist. 2 nd ed. Stanford: Stanford University Press 1959; p: 233-47.
|
| 31. | Weiland FJ, Bantleon HP. Treatment of Class II malocclusions with the Jasper Jumper appliance-a preliminary report. Am J Orthod Dentofacial Orthop 1995;108:341-50.
|
| 32. | Stockli PW, Willert HW. Tissue reactions in the temporomandibular joint resulting from anterior displacement of the mandible in the monkey. Am J Orthod 1971;60:142-55.
|
| 33. | Birkebaek L, Melsen B, Terp S. A laminographic study of the alterations in the temporo-mandibular joint following activator treatment. Eur J Orthod 1984;6:257-66.
[PUBMED] |
| 34. | Woodside DG, Metaxas A, Altuna G. The influence of functional appliance therapy on glenoid fossa remodeling. Am J Orthod Dentofacial Orthop 1987;92:181-98.
[PUBMED] |
| 35. | Arat ZM, Gokalp H, Erdem D, Erden I. Changes in the TMJ disc-condyle-fossa relationship following functional treatment of skeletal Class II division 1 malocclusion: A magnetic resonance imaging study. Am J Orthod Dentofacial Orthop 2001;119:316-9.
|
| 36. | Kucukkeles N, Ilhan I, Orgun IA. Treatment efficiency in skeletal class II patients treated with the jasper jumper. Angle Orthod 2007;77:449-56.
|
| 37. | Stuckli N, Ingervall B. The use of the Jasper Jumper for the correction of Class II malocclusion in the young permanent dentition. Eur J Orthod 1998;20:271-81.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7]
[Table 1], [Table 2]
|











 Search Pubmed for
Search Pubmed for