|
 
 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 2
| Issue : 1 | Page : 46-49 |
|
An alternative choice: Obtaining space for a canine with asymmetric fan type expansion appliance
Ebubekir Toy, Eyup Burak Kucuk
Department of Orthodontics, Faculty of Dentistry, Inonu University, Malatya, Turkey
| Date of Web Publication | 29-Jan-2014 |
Correspondence Address:
Ebubekir Toy
Department of Orthodontics, Faculty of Dentistry, Inonu University, 44280 Malatya
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.125929

A 12-year old female patient presented with her unesthetic appearance while smiling. The patient had a vestibule positioned upper-left canine, beside mesofacial face type, flat profile, Class II molar and canine relationships clinically. Dental crowding was 7.8 mm in the upper arch and 4.1 mm in the lower. Treatment plan included to obtain space for the upper-left canine using a modified fan type expansion appliance, followed by comprehensive fixed orthodontic treatment. The aim of this case report is to present a non-extraction treatment of a patient using asymmetric fan type expansion appliance. Keywords: Fan type expansion, non-extraction treatment, removable appliance
How to cite this article:
Toy E, Kucuk EB. An alternative choice: Obtaining space for a canine with asymmetric fan type expansion appliance. J Orthod Res 2014;2:46-9 |
How to cite this URL:
Toy E, Kucuk EB. An alternative choice: Obtaining space for a canine with asymmetric fan type expansion appliance. J Orthod Res [serial online] 2014 [cited 2018 Apr 5];2:46-9. Available from: http://www.jorthodr.org/text.asp?2014/2/1/46/125929 |
| Introduction | |  |
Dental crowding is one of the most common orthodontic problems in modern postindustrial societies, occurring as a result of increased processing of foods. [1] Since crowded teeth cause unaesthetic smiles, children and their parents seek orthodontic treatment. Dental crowding was described by Nance [2] as a malocclusion resulting from the difference between the space needed in the dental arch and the space available in that arch.
There are various methods to solve dental crowding in orthodontic practice, such as either orthodontic treatment with extraction [3],[4] or non-extraction treatment with distalization [5] and/or expansion. [6],[7] Palatal expansion, whether rapid or slow, is a way to gain space in the upper arch. Some cases require expansion in only anterior region of the maxilla when the upper dental arch is constricted in the anterior or V-shaped. Fan type expansion appliance is one of the preferred approaches for the dental crowding cases to have more space in the maxillary inter-canine distance. This expansion design was firstly used by Schellino [8] in 1996 and was named "Ragno." The appliance allows a "fan opening" in the upper dental arch.
We applied a modification in fan type expansion appliance and placed the fan type screw asymmetrically in the acrylic plate to open space for the canine. The aim of this case report is to present a non-extraction treatment of a patient with a vestibule positioned upper canine using an asymmetric fan type expansion appliance.
| Case Report | | |
Diagnosis and Etiology
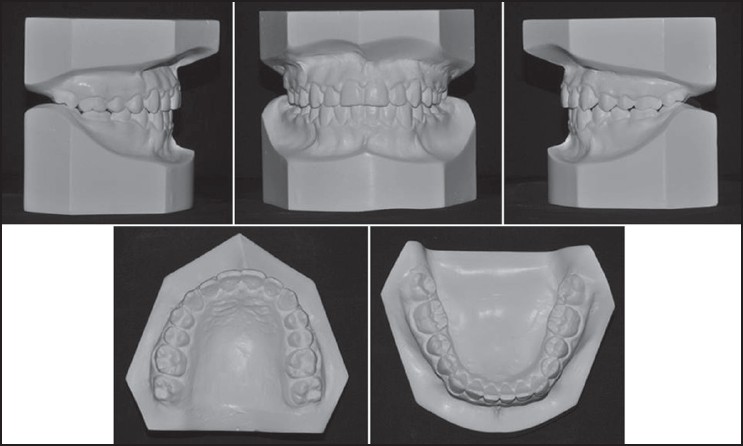
A 12-year-old female patient referred to our department with her unesthetic appearance compliant while smiling. The intraoral examination showed that the patient had a vestibule positioned upper-left canine, Angle Class II molar and canine relationships. The maxillary arch was V-shaped. The upper midline was deviated toward the left side and lower midline towards the right side. The facial analysis showed a symmetric face, a balanced facial pattern, an asymmetric smile, mesofacial face type and flat profile [Figure 1]. Since early loss of the deciduous molars resulted in mesial tipping of the left buccal segment, there was not adequate space for the upper left permanent canine; therefore, the canine placed in high vestibule position. Model analysis revealed that there were arch length discrepancies of −7.8 mm in the maxillary arch and −4.1 mm in the mandibular arch. Overjet and overbite were 2 and 2.5 mm, respectively [Figure 2].
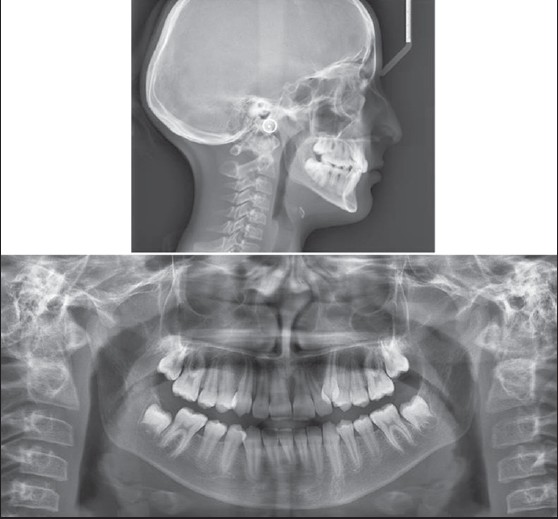
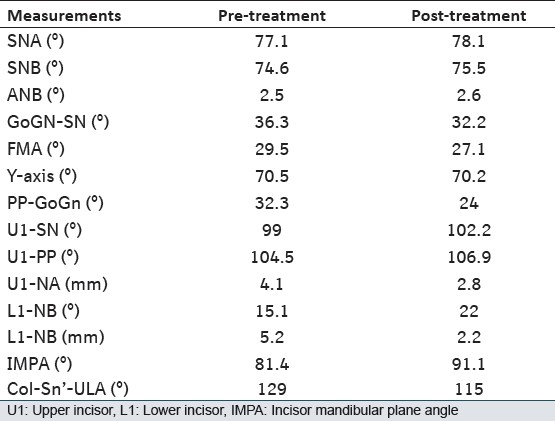
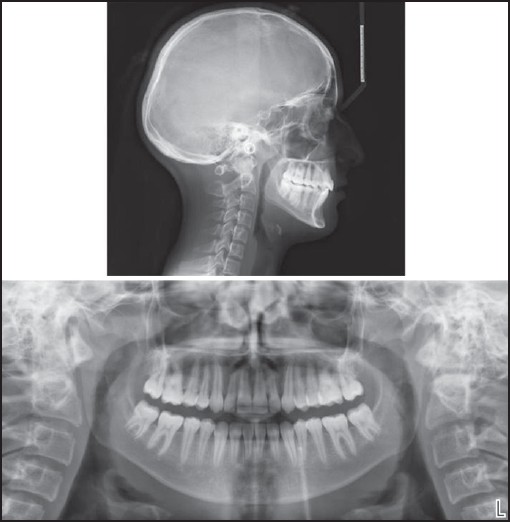
The initial cephalometric analysis showed skeletal Angle Class I malocclusion: ANB, 2.5°; retroclined maxillary and mandibular incisors [Upper incisor (U1)-SN, 99°; U1: NA, 4.1 mm and 21°; lower incisor (L1): NB, 5.2 mm and 21.9°; incisor mandibular plane angle (IMPA), 81.4°]; mandibular plane, 36.3° and FMA, 29.5° [Figure 3], [Table 1].
The radiographic findings showed no pathology in the periapical area and no root dilacerations.
The patient was physically healthy and had no history of medical diseases or dental trauma.
Treatment Objectives
The treatment objectives were: (1) to gain space for the maxillary left canine; (2) to drift the upper left canine to the dental arch; (3) to correct upper and lower midline deviations; (4) to create a stable functional occlusion, and (5) to establish an esthetic smile.
Treatment Alternatives
- Gaining space for upper left canine using fan type expansion appliance, and then bringing upper left canine into its proper position by applying fixed orthodontic therapy.
- Extraction of the two maxillary first premolars; thus, upper midline may be easily corrected.
- Extraction of the left maxillary canine and reshaping the palatal cuspid of left premolar to recreate an ideal canine contour.
- Both orthopedic maxillary expansion and orthodontic space opening for upper left canine.
Treatment Plan
After we discussed the treatment alternatives with patient and her parents, they chose the first alternative. 2-stage orthodontic treatment was executed; the first stage included obtaining space for upper-left canine using the asymmetric fan type expansion appliance, followed by inactive period for 6 weeks for stabilization. Then, comprehensive fixed orthodontic treatment, as a second stage, was carried out to achieve Class I molar and canine relationships and a pleasant smile, as well as well-balanced occlusion including finishing and final detailing procedures.
Treatment Progress
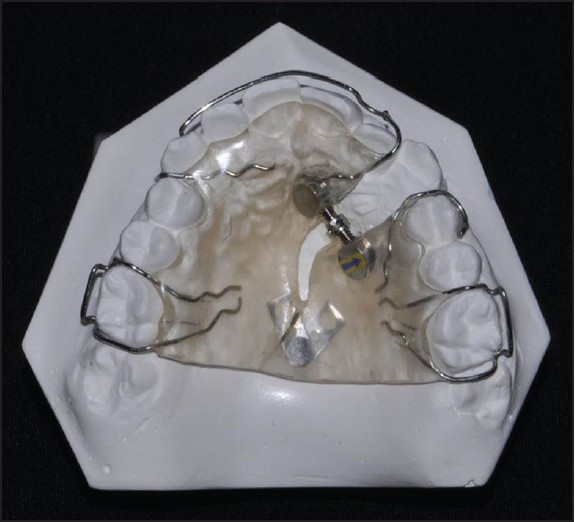
Space gaining was accomplished using a modified fan type expansion appliance [Figure 4]. In this appliance, the fan type screw was placed asymmetrically in the acrylic plate to obtain space for the canine. The activation rate was prescribed to be one-quarter of a turn per 4 days. [9] Within 3 months, enough space was obtained for displaced canine [Figure 5] and [Figure 6].
The appliance was left in the mouth passively for 6 weeks to maintain the opening and to allow the canine to drift through the available space spontaneously. After this time, transpalatal arch was placed for molar anchorage. Initial leveling and alignment was achieved with pre-adjusted appliances. The leveling began with a 0.012 in nickel-titanium (NiTi) arch wire. 0.014, 0.016 and 0.016 × 0.016 in NiTi arch wires were placed, respectively. After leveling of the maxillary arch, mandibular arch was bonded. Final alignment was completed in both dental arches using 0.016 × 0.022 in up to 0.017 × 0.025 in stainless steel arch wires. Inter maxillary elastics were used to obtain ideal canine and molar relationships. Ideal overbite and overjet were established. Treatment was completed in a total of 21 months. The fixed appliances were removed and Essix retainers were placed in both arches. Final records including extraoral and intraoral photographs, dental casts, panoramic and lateral cephalometric radiographs were taken [Figure 7], [Figure 8] and [Figure 9].
Treatment Results
Enough space was acquired for upper left canine using the asymmetric fan type expansion appliance, and the high vestibule positioned maxillary left canine was brought into its proper position. At the end of the fixed orthodontic treatment, the patient had a symmetric and beautiful smile [Figure 7].
A bilateral Class I occlusion with ideal overjet and overbite was achieved with the protrusion effect of asymmetric fan type expansion appliance and intraoral elastics. Upper and lower midlines were matched the facial midline and a satisfactory interdigitation was provided [Figure 8].
The final panoramic radiograph indicated that there were not only proper root alignment and reasonable root length, but also no pulp obliteration, periapical radiolucency, or apparent root resorption. The final cephalometric analysis showed that ANB was in the normal values (ANB: 2.6°), and retrusion of the maxillary and mandibular incisors was corrected (U1-SN: 102.2°; U1-PP: 106.9°; IMPA: 91.1°; L1: NB, 22°); nasolabial angle was decreased (Col-Sn'-ULA: 115°); the palatal-mandibular plane angle (PP-GoGn) of 24° was within normal values [Figure 9], [Table 1]. Total and regional superimpositions showed that the mandible had a favorable direction of growth [Figure 10].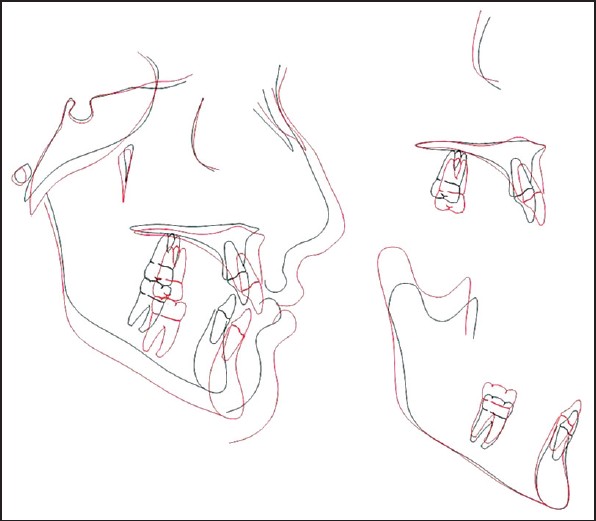 | Figure 10: Total superimposition and regional superimposition (black, pre-treatment; red, post-treatment)
Click here to view |
As a conclusion, space gaining with asymmetric fan type expansion appliance was achieved in a short time without extraction. Oral hygiene of our patient was very good expectedly during appliance use. A well-balanced occlusion was established and asymmetric smiling was eliminated at the end of the fixed orthodontic treatment. The asymmetric fan type expansion appliance may be a useful approach to open space for a canine in cases suitable for removable appliance treatment. This appliance provides a great advantage to obtain space, increases patient's comfort and eases fixed therapy in appropriate cases.
| References | | |
| 1. | von Cramon-Taubadel N. Global human mandibular variation reflects differences in agricultural and hunter-gatherer subsistence strategies. Proc Natl Acad Sci U S A 2011;108:19546-51. 
[PUBMED] |
| 2. | Nance HN. The limitations of orthodontic treatment; mixed dentition diagnosis and treatment. Am J Orthod 1947;33:177-223.
[PUBMED] |
| 3. | Boley JC, Mark JA, Sachdeva RC, Buschang PH. Long-term stability of Class I premolar extraction treatment. Am J Orthod Dentofacial Orthop 2003;124:277-87.
[PUBMED] |
| 4. | Taner-Sarisoy L, Darendeliler N. The influence of extraction orthodontic treatment on craniofacial structures: Evaluation according to two different factors. Am J Orthod Dentofacial Orthop 1999;115:508-14.
[PUBMED] |
| 5. | Toy E, Enacar A. The effects of the pendulum distalising appliance and cervical headgear on the dentofacial structures. Aust Orthod J 2011;27:10-6.
[PUBMED] |
| 6. | Defraia E, Marinelli A, Baroni G, Tollaro I. Dentoskeletal effects of a removable appliance for expansion of the maxillary arch: A postero-anterior cephalometric study. Eur J Orthod 2008;30:57-60.
[PUBMED] |
| 7. | Doruk C, Bicakci AA, Basciftci FA, Agar U, Babacan H. A comparison of the effects of rapid maxillary expansion and fan-type rapid maxillary expansion on dentofacial structures. Angle Orthod 2004;74:184-94.
[PUBMED] |
| 8. | Schellino E, Modica R, Benech A, Modaro E. REM: la vite ragno secondo Schellino e Modica. Boll Interm Orthod. Leone 1996;55:36-9.
|
| 9. | Brunetto M, Andriani Jda S, Ribeiro GL, Locks A, Correa M, Correa LR. Three-dimensional assessment of buccal alveolar bone after rapid and slow maxillary expansion: A clinical trial study. Am J Orthod Dentofacial Orthop 2013;143:633-44.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9], [Figure 10]
[Table 1]
|















 Search Pubmed for
Search Pubmed for