|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 2
| Issue : 1 | Page : 4-10 |
|
Tooth size and arch parameter discrepancies among different malocclusions in young permanent dentition of 13-15-year-old school children of Nalgonda District-South Indian population
Mohammadi Begum1, Santhosh Kumar Goje2, Arjun Karra3, Sreevalli Mohan1
1 Department of orthodontics and dentofacial orthopeadics, Drs. Sudha and Nageswara Rao Pinnamineni Siddhartha Institute of Dental Sciences, Gunnavaram, Vijayawada, India
2 Department of orthodontics and dentofacial orthopeadics, KM Shah Dental College and Hospital, Sumandeep Vidyapeeth University, Piparia, Wagodia, Vadodara, Gujarat, India
3 Department of orthodontics and dentofacial orthopeadics, Army College of Dental Sciences, Secunderabad, Andhra Pradesh, India
| Date of Web Publication | 29-Jan-2014 |
Correspondence Address:
Mohammadi Begum
Drs. Sudha and Nageswara Rao Pinnamineni Siddhartha Institute of Dental Sciences, Gunnavaram, Vijayawada - 521 286, Andhra Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.125901

Purpose: The objective of this study was to evaluate the presence of tooth material and arch length discrepancies of children in Nalgonda district, Andhra Pradesh, South India, in an age range of 13-15 years. Materials and Methods: Children aged 13-15 years who fulfilled the inclusion and exclusion criteria were selected for a sample of 200 children. A digital caliper
was used for measuring the tooth and arch widths. Results: Significant tooth size differences were found between males and females and among different malocclusion groups. In the Class I malocclusion group, the mandibular canines were significantly smaller in females than that in males (P < 0.01). Class II div 1 group showed relatively narrower intercanine width compared with other groups. Class III occlusal pattern showed relatively larger sized teeth compared with the other occlusal groups. There was no statistically significant difference in the anterior and overall ratio in all the malocclusion groups. Conclusion: The following conclusions are drawn from the study:
- The maxillary central and lateral incisors presented significant variability.
- No significant sex differences were shown for Bolton's overall ratio and anterior ratio.
- Treatment planning should always take into consideration the discrepancy of the tooth size ratios and should include compensating esthetic procedures such as composite bonding, prosthetic reconstruction or reproximation.
Keywords: Arch width, arch length, Bolton′s ratio, tooth material-arch length discrepancy
How to cite this article:
Begum M, Goje SK, Karra A, Mohan S. Tooth size and arch parameter discrepancies among different malocclusions in young permanent dentition of 13-15-year-old school children of Nalgonda District-South Indian population. J Orthod Res 2014;2:4-10 |
How to cite this URL:
Begum M, Goje SK, Karra A, Mohan S. Tooth size and arch parameter discrepancies among different malocclusions in young permanent dentition of 13-15-year-old school children of Nalgonda District-South Indian population. J Orthod Res [serial online] 2014 [cited 2018 Mar 17];2:4-10. Available from: http://www.jorthodr.org/text.asp?2014/2/1/4/125901 |
| Introduction | |  |
Oral health is an essential component of health throughout life. The oral cavity is associated with the development of a healthy personality, perceptions and the overall experiences of pleasure. According to Dr. Dale, [1] the main cause of malocclusion is the delayed eruption of permanent teeth, which could be basically because of retained deciduous teeth. We know since ages that malocclusion has been affecting the human population and it is considered to be the next forerunner of dental caries affecting children and adults. It is a known fact that the tooth size discrepancy is associated with detrimental effects such as caries, periodontal problems and temporomandibular joint problems and, ultimately, produces lowered self-esteem. It is therefore important to identify these problems at the earliest and treat them to overcome the interarch and intraarch tooth discrepancies by either addition or removal of tooth structures to open or close the spaces in the same or the opposing arches, as there should be a specific dimensional relationship between the maxillary and the mandibular teeth to maintain proper interdigitation, overjet and overbite.
It is a known fact that interarch tooth size relationship differs due to differences in the tooth sizes among males and females and its variation with the population and the ethnic region. Bolton [2] revealed that proper occlusal interdigitation in the finishing stages of orthodontic treatment is directly related to the correct maxillary and mandibular tooth size relationship. He computed the specific ratios of the mesiodistal tooth widths that must exist between the maxillary and mandibular teeth from both canine to canine and first molar to first molar so as to obtain an optimum occlusion. The sizes of the teeth and the bony bases have been the fundamental factors to result in either crowding or spacing in the dental arches. It is also confirmed that heredity, gender differences and secular trends have been the main contributing factors for the tooth size variations. The effect of tooth size and arch length dimensions on crowding and spacings has been investigated by various researchers in the past.
Aims and Objectives
To estimate the mesiodistal tooth size including the first molar in both the upper and the lower arches, arch widths, arch lengths and Bolton's anterior and overall ratio in the selected sample casts and determination of the effect of sexual dimorphism on the size of the tooth or the teeth in the study sample.
| Materials and Methods | | |
This cross=sectional study was intended to assess tooth size, arch length and arch width discrepancies along with Bolton's tooth size discrepancies and their comparisons in all the four malocclusion groups, including Angle's Class I, Class II div 1, Class II div 2 and Class III, in a sample size of 200 school children in age range of 13-15 years, including both boys and girls from Nalgonda district of Andhra Pradesh, South India.
Inclusion Criteria
The criteria for inclusion in the study were:
- Children in the age range of 13-15 years
- Children with erupted second permanent molar
- Children who have never been orthodontic patients
- Children with no systemic problems or syndromic patients.
Method of Study
The selected school children after following the inclusion criteria were included in the sample and their upper and lower jaw impressions were made in an alginate impression material. The assessment of mesiodistal tooth size of all upper and lower jaw teeth was done by using a digital caliper [Figure 1]. The arch length assessment was done by using brass wire from the mesial wall of the first molar to the mesial wall of the first molar of the contralateral side [Figure 2]. The arch width was checked at the canine, first premolar, second premolar and first molar at three anatomical points, i.e. the width was measured from the buccal cusp tip to the buccal cusp tip, from central fossa to the central fossa and from the lingual cusp tip to the lingual cusp tip in both the arches using a digital caliper [Figure 3].
The statistical parameters used in this study were mean, standard deviation, Student's t-test, Paired t-test and ANOVA. In order to determine whether there is sexual dimorphism in the incidence of intermaxillary tooth size discrepancies, a Student's t-test was performed for each malocclusion group. The software of the above statistical analysis was SPSS (Version 19) and the level of significance was P <0.05. All the measurements were performed by the same investigator. Sixty study casts (20 from each group) were randomly selected from the sample and remeasured at 2-week intervals by the same individual investigator using the Paired t-test to check the intraexaminer accuracy in both maxillary and mandibular measurements. Since all the P-values were greater than 0.05, there was no significant difference in the first and second measurements. The Houston's coefficient of reliability was 0.91. Analysis of variance (ANOVA) was performed to compare intermaxillary tooth size discrepancies among different malocclusion groups and to compare the mean ratios of the Bolton's analysis.
Armamentarium
- Hydrocolloid impression material
- Rubber bowl and spatula
- Water
- Impression trays (plastic and stainless steel)
- Dental stone
- Plaster of Paris
- Digital caliper
- Brass wire
- Paper sheet with tabular column [Figure 4].
 | Figure 4: Alginate impression material, mixing bowl and spatula, impression trays, dental stone, hand gloves and digital Vernier caliper
Click here to view |
| Results | | |
Based on Different Malocclusion Groups
When the tooth size was compared among the different malocclusion groups, it was found that Class II div 2 group showed significantly larger sized maxillary lateral incisors than the other groups, except for Class III (P < 0.01). The Class III group showed significantly larger sized maxillary central incisors compared with the other groups (P < 0.05). The Class II div 2 group showed larger sized maxillary canines compared with the other groups (P < 0.01). The maxillary molars in the Class II div 2 group were significantly larger than the Class III group maxillary molars (P < 0.01). In the mandibular teeth, the mandibular first molars were found to be larger in mesiodistal width in the Class III group and the Class II div 2 group compared with the other groups (P < 0.01). The mandibular second premolars in the Class III group were found to be larger than the Class I group (P < 0.05) [Table 1] and [Table 2]. | Table 1: Differences in the Mesiodistal widths in different malocclusion groups in Maxillary arch
Click here to view |
 | Table 2: Differences in the Mesiodistal widths in different malocclusion groups in Mandibular arch
Click here to view |
Based on Bolton's Tooth Ratios
The different malocclusion groups showed no significant differences among themselves when Bolton's overall and anterior ratios were assessed [Table 3].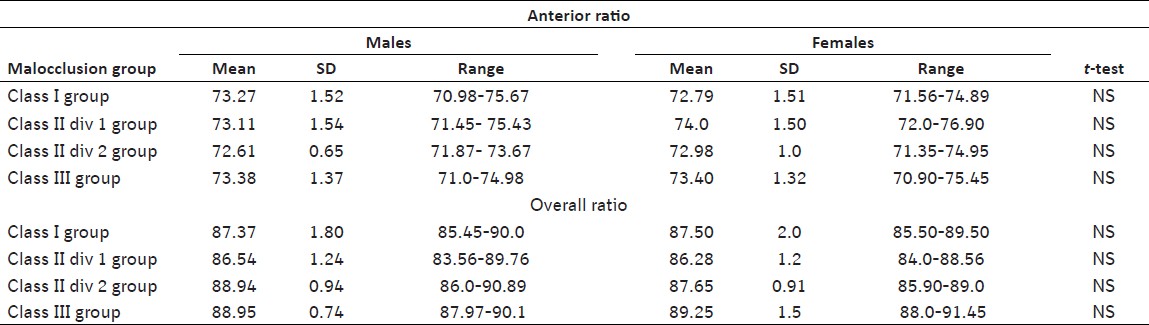 | Table 3: Bolton's anterior and overall tooth size ratios for both males and females with different malocclusion groups
Click here to view |
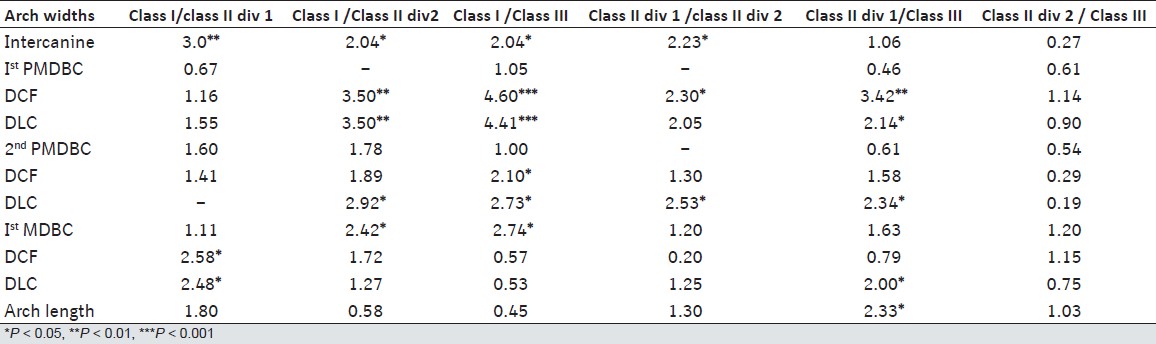
Based on Arch Length
The Class III malocclusion group showed smaller sized maxillary arch lengths compared with the other groups. The Class II div 1 group showed an increased maxillary arch length. The Class I group showed smaller sized mandibular arch lengths compared with the other groups [Table 4] and [Table 5].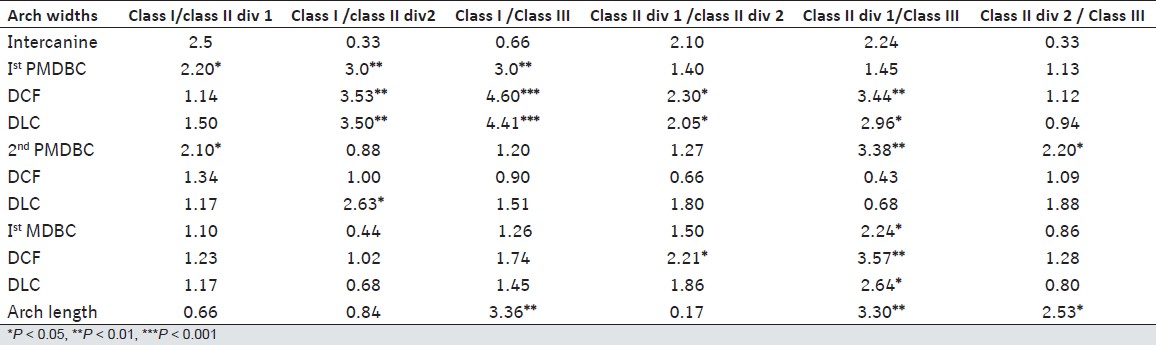 | Table 4 : Differences between Arch lengths and Arch widths of different teeth in different malocclusion groups in Maxillary arch
Click here to view |
 | Table 5 : Differences between Arch lengths and Arch widths of different teeth in different malocclusion groups in Mandibular arch
Click here to view |
Based on the Arch Widths
It was found that the Class II div 1 group showed significantly smaller sized arch width at the intercanine region. The Class III group followed by the Class II div2 group showed smaller arch widths at the premolar regions in the maxilla. The Class II div 1 group showed lowered values at the intermolar region measured at the three anatomical points, buccal cusps, central fossae and the palatal cusps regions. This group was also found to be having significantly smaller values at the mandibular intercanine region than the other malocclusion groups. The mandibular first and second premolar widths were found to be lower at the buccal cusps in the Class II div 1 occlusion pattern, at the level of central fossae in the Class II div 1 occlusion pattern and at the level of lingual cusps in both Class II div 1 and Class II div 2 malocclusion groups. The intermolar widths were found to be smaller in the Class I group at the buccal cusps, central fossae and lingual cusps, followed by the Class II div 1 and Class II div 2 occlusion patterns [Table 4] and [Table 5].
| Discussion | | |
Over the years, it is a known and proven fact that a tooth size difference exists in different population groups and that this has contributed to the prevalence of interarch tooth size relationship, as the tooth size differences never happen systematically. [3],[4],[5],[6],[7] It is a very much accepted fact that heredity, secular trends, gender differences and ethnicity do affect the tooth size in both the arches. [8],[9],[10],[11],[12],[13],[14],[15] The aim of the present study was to assess and confirm the facts that the tooth size, arch width and arch length do have reflections of the heredity, gender differences and ethnicity on them when measured in both the arches of the young permanent dentition of Nalgonda district of Andhra Pradesh, Southern India, showing all four types of malocclusions.
The mesiodistal tooth width of the maxillary teeth showed greater variability than the mandibular teeth, with the first molar dimensions having the greatest variability. The size of the maxillary lateral incisor also was highly variable. In addition, the individual tooth size data reported by Santoro et al.[15] imply high variability for the maxillary first molar and the lateral incisor, and this agrees with the present study. This suggests that these teeth could be responsible for the incongruity in the anterior ratio and should be examined clinically at the beginning of the treatment to detect any major size and shape variations. The values obtained in this study closely resemble the data available for the Dominican American, Dominican and North American groups. Most of the values were slightly lower than those of the other population groups. These differences could be attributed to the differences in the measurement techniques among these studies or even to different nutrition regimens in these population groups.
This study revealed no significant differences of Bolton's ratio among the different malocclusion groups. This finding is similar to some studies done on other populations; however, in a Chinese population, the study revealed a larger Bolton's ratio for the Class III occlusal pattern. [16] This study revealed that the Class II div 1 group had a smaller value for intercanine width, which is in correlation with the findings of Staley et al.,[17] which revealed larger intercanine width for normal occlusion than in the Class II div 1 group, although Sayin and Turkkahraman [18] reported larger intercanine width in the Class II div 1 group than in the Class I group.
This study revealed the intercanine width in the Class III group to be larger than that in the Class II div 1 and Class II div 2 groups. The arch width at the interpremolars and intermolar regions was significantly smaller in the Class II div 1 group when compared with the other groups; this finding is similar with some previous studies. [19],[20] Costalos et al. and Rudolph et al.[21],[22] compared the Class I, Class II and Class III malocclusion groups in different populations. They found that maxillary arch length in the Class II div 1 group were significantly larger than that in the Class II div 2 group, which was an expected result, considering the proclination of the maxillary central incisors in the Class II div 1 group compared with the Class II div 2 group. This finding was similar to our results. In the mandibular arch, both the Class II div 1 and the Class II div 2 arches were shorter than that of the Class III malocclusion group, showing that the growth potential of the mandible in Class III group is greater. These findings were to be similar with other studies. [23],[24]
Studies carried out on a Chinese population by Nie and Lin [25] found that tooth size is not affected by sexual dimorphism, although different malocclusion groups show variability in their anterior or posterior teeth size, which could be found in the maxillary or mandibular arch. This is found to be in agreement with the present study.
Crosby and Alexander, [26] showed that there exist no differences in Bolton's overall and anterior ratios among different malocclusion groups. This was found to be in agreement with our present study. One more study by Freeman et al.[27] also confirmed this finding by reporting that 157 orthodontic patients with different occlusal patterns had nearly identical mean overall and anterior Bolton's ratio.
| Summary and Conclusion | | |
The correct tooth size relationship between the maxillary and mandibular teeth is an important factor to achieve a proper intercuspation during the final stage of orthodontic treatment.
The relationship between the sizes of the mandibular and maxillary teeth depends on specific population and gender. This study indicated that a population-specific standard is necessary for the clinical assessments. Significant gender differences were shown for the overall ratio. These differences could be explained based on the fact that males tend to show relatively larger mandibular arch segment compared with females, and that females tend to have smaller teeth size compared with males. The Class III malocclusion group showed relatively larger teeth size compared with the other occlusion categories and a relatively larger mandibular arch, which might have contributed toward the interarch and intergroup variations in Bolton's ratio. The Class II div 1 group showed a relatively narrower intercanine width compared with the other groups as these group children show proclined maxillary incisors resulting in a longer maxillary arch length in this malocclusion group. The Class III malocclusion group showed larger intercanine widths in the mandibular arch, which was significant when compared with the other malocclusion groups. The maxillary arch was shorter in the Class II div 1 than in the Class II div 2 and Class III malocclusion. The mandibular arch was significantly larger in the Class III group than in the Class II div 1 and Class II div 2 groups, which contributes to its increased growth potential.
The following conclusions are drawn from the present study:
- The maxillary central and the lateral incisors presented significant variability among the different malocclusion groups.
- Bolton's overall and anterior ratios showed no significant variations in the different malocclusion groups.
- The Class II div 1 group showed a relatively narrower intercanine width, along with an increased arch length, which is always expected, when compared with the other groups.
- The Class III occlusal pattern showed relatively larger sized teeth compared with the other occlusal groups.
- The Class III group showed a larger intercanine width in the mandibular arch, which was significant when compared with other the malocclusion groups.
Clinical Implications of the Present Study
Treatment planning should always take into consideration the discrepancy of the tooth size ratios, and should include compensating esthetic procedures such as composite bonding, prosthetic reconstruction, stripping and crown recontouring. The final results of any extraction case could be compromised if the tooth size information is lacking.
As the present study has provided relevant information regarding the individual variations in different parameters such as tooth size, Bolton's ratio, arch length and arch width in both males and females having different occlusal relationships, the results suggest that this data would be helpful in treatment planning in adolescent children. The data also provide information regarding the tooth size discrepancy between the maxillary and mandibular teeth, which may be one of the important factors in the cause of malocclusion, especially in Class II and Class III malocclusions. In order to obtain optimal and stable treatment results, Bolton's analysis should be taken into consideration when diagnosing, planning and predicting prognosis in clinical orthodontics.
Scope for Future Studies: Dental anomalies in tooth size, number or shape must also be taken into consideration along with the buccolingual tooth proportion. The intra- and interexaminer calibration should be developed to provide more consistent and reliable results. 3D models can be used for more precise and accurate measurements in all three planes of space. The relationship of malocclusion to the skeletal pattern can also be taken into consideration to arrive at more statistically significant differences in the prevalence of the tooth size discrepancies among different malocclusion groups. Certainly, further work is needed to explain the probable existing racial differences for intermaxillary tooth size discrepancies in the different malocclusion categories.
| References | | |
| 1. | Dale G. Guidance of Occlusion: Serial Extraction. In: Graber YM, Swain BF, editors. Orthodontic Current Principles and Technique. St. Louis: C. V. Mosby Company; 1985. p. 284-95. 
|
| 2. | Stifter J. A study of Pont′s, Howe′s Rees Neff, and Bolton analysis on class I adult dentitions. Angle Orthod 1958;28:215.
|
| 3. | Rosenzweig KA. Tooth form as a distinguishing trait between sexes and human populations. J Dent Res 1970;49 Suppl:1423-6.
|
| 4. | Merz ML, Isacson RJ, Germane N, Rubenstein LK. Tooth diameters and arch perimeters in a black and white population. Am J Orthod Dentofacial Orthop 1991;100:53-8.
|
| 5. | Paredes V, Gandia JL, Cibrian R. Do Bolton′s ratios apply to a Spanish population. Am J Orthod Dentofacial Orthop 2006;129:428-30.
[PUBMED] |
| 6. | Uysal T, Sari Z. Intermaxillary tooth size discrepancy and mesiodistal crown dimensions for a Turkish population. Am J Orthod Dentofacial Orthop 2005;128:226-30.
[PUBMED] |
| 7. | Akyalcin S, Dogan S, Dincer B, Erdinc AM, Oncað G. Bolton tooth size discrepancies in Skeletal class I individuals presenting with different Dental Angle′s classifications. Angle Orthod 2006;76:637-43.
|
| 8. | Basaran G, Selek M, Hamanui O, Akkuº Z. Intermaxillary Bolton tooth size discrepancies among different malocclusion groups. Angle Orthod 2006;76:226-30.
|
| 9. | Johe RS, Steinhart T, Sado N, Greenberg B, Jing S. Intermaxillary tooth size discrepancies in different sexes and malocclusion Groups. Am J Orthod Dentofacial Orthop 2010;137:145-51.
|
| 10. | Malkoç S, Basçiftçi FA, Nur M, Catalbas B. Maxillary and mandibular tooth sizes among different malocclusions in a sample of the Turkish population. Eur J Orthod 2011;33:592-6.
|
| 11. | Lavelle CL. Maxillary and mandibular tooth size in different racial groups and in different occlusal categories. Am J Orthod 1972;61:29-37.
[PUBMED] |
| 12. | Smith SS, Buschang PH, Watanabe E. Interarch tooth size relationships of 3 populations: ′′Does Bolton′s analysis apply?′′Am J Orthod Dentofacial Orthop 2000;117:169-74.
|
| 13. | Ta TA, Ling JY, Hagg U. Tooth-size discrepancies among different occlusion groups of southern Chinese children. Am J Orthod Dentofacial Orthop 2001;120:556-8.
|
| 14. | Al-khateeb SN, Abu Alhaija ES. Tooth size discrepancies and Arch parameters among different malocclusions in a Jordanian sample. Angle Orthod 2006;76:459-65.
|
| 15. | Santoro M, Ayoub ME, Pardi VA, Cangialosi TJ. Mesiodistal crown dimensions and tooth size discrepancy of the permanent dentition of Dominican Americans. Angle Orthod 2000;70:303-7.
|
| 16. | Puneky PJ, Sadowsky C, BeGole EA. Tooth morphology and the lower incisor alignment many years after orthodontic therapy. Am J Orthod 1984;86:299-305.
|
| 17. | Staley RN, Stuntz WR, Peterson LC. A Comparison of arch widths in adults with normal occlusion and adults with class II div 1 malocclusion. Am J Orthod 1985;8:163-9.
|
| 18. | Sayin MO, Turkkahraman H. Comparison of dental arch and alveolar widths of patients with class II div 1 malocclusion and subjects with ideal occlusion. Angle Orthod 2004;74:356-60.
|
| 19. | Stevens DR, Flores-Mir C, Nebbe B, Rabound DW. Validity, Reliability and Reproducibility of plaster vs digital study models: Comparison of peer assessment rating, Bolton′s analysis and their constituent measurements. Am J Orthod Dentofacial Orthop 2006;129:794-803.
|
| 20. | Melgaco CA, Araujo MT, Ruellas AC. Applicability of Moyer′s and Tanaka-Johnston′s method for mixed dentition analysis in Brazilian individuals. Angle Orthod 2006;76:644-9.
|
| 21. | Costalos PA, Sarraf K, Cangialosi TJ, Efstratiadis S. Evaluation of the accuracy of digital model analysis for the American Board of Orthodontics objective grading system for dental casts. Am J Orthod Dentofacial Orthop 2005;128:624-9.
|
| 22. | Rudolph DJ, Dominguez PD, Ahn K, Thinh T. The use of tooth thickness in predicting intermaxillary tooth size discrepancies. Angle Orthod 1998;68:133-40.
|
| 23. | Yoo YK, Kim NI, Lee HK. A study on the prevalence of malocclusion in 2378 Yonsei University students. Korean J Orthod 1971;2:35-40.
|
| 24. | Mitani H, Sato K, Sugawara J. Growth of mandibular prognathism after pubertal growth peak. Am J Orthod Dentofacial Orthop 1993;104:330-6.
|
| 25. | Nie Q, Lin J. Comparison of maxillary tooth size discrepancies among different malocclusion groups. Am J Orthod Dentofacial Orthop 1999;116:539-40.
|
| 26. | Crosby DR, Alexander CG. The occurrence of tooth size discrepancies among different malocclusion groups. Am J Orthod Dentofacial Orthop 1989;95:457-61.
|
| 27. | Freeman JE, Maskeroni AJ, Lorto L. Frequency of Bolton tooth size discrepancies among Orthodontic patients. Am J Orthod Dentofacial Orthop 1996;110:24-7.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5]
|













 Search Pubmed for
Search Pubmed for