|
 
 |
|
CASE REPORT |
|
|
|
| Year : 2012 | Volume
: 18
| Issue : 3 | Page : 356-358 |
| |
Proteus syndrome: A rare case report
Keerthi Talari, Praveen Kumar Arinaganhalli Subbanna, Deepak Amalnath, Subrahmanyam Dharanitragada Krishna Suri
Department of Medicine, Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry, India
| Date of Web Publication | 4-Mar-2013 |
Correspondence Address:
Praveen Kumar Arinaganhalli Subbanna
Department of Medicine, JIPMER, Pondicherry - 605 006
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.108036

 Abstract Abstract | | |
Proteus syndrome (PS) is a rare hamartomatous disorder characterized by various cutaneous and subcutaneous lesions, including vascular malformations, lipomas, hyperpigmentation, and several types of nevi. Partial gigantism with limb or digital overgrowth is pathognomonic of PS. We report a rare case of PS in a 50-year-old man who presented with inferior wall myocardial infarction and was incidentally detected to have hypertrophy of index and middle fingers of both the hands.
Keywords: Gigantism, hamartoma, mosaicism, proteus syndrome
How to cite this article:
Talari K, Subbanna PA, Amalnath D, Krishna Suri SD. Proteus syndrome: A rare case report. Indian J Hum Genet 2012;18:356-8 |
How to cite this URL:
Talari K, Subbanna PA, Amalnath D, Krishna Suri SD. Proteus syndrome: A rare case report. Indian J Hum Genet [serial online] 2012 [cited 2016 Jun 1];18:356-8. Available from: http://www.ijhg.com/text.asp?2012/18/3/356/108036 |
| Introduction | |  |
Proteus syndrome (PS) is a rare and sporadic disorder that causes postnatal overgrowth of tissues in a mosaic pattern. [1] It produces multifocal overgrowth of tissue derived from any of the three germinal layers. This causes a complex disorder with multisystem involvement and great clinical variability. The complications of PS include, progressive skeletal deformities, invasive lipomas, benign and malignant tumors, and deep venous thrombosis with pulmonary embolism. [1] We report a rare case of PS that presented with hypertrophy of index and middle finger without any other abnormalities or complications.
| Case Report | | |
A 50-year-old farmer presented to our emergency services with anginal pain. ECG revealed inferior wall myocardial infarction (MI). As patient presented in window period he was thrombolysed. Incidentally we noticed that he had enlarged index and middle fingers of both hands and thumb of right hand [Figure 1]. On probing patient revealed that it was present since childhood with onset around the age of 5 years and gradual progression over years to the present size. No similar tissue growth in other parts of the body and there was no one in the family with similar features. On examination there was hypertrophy of the involved fingers with limitation of movements. His systemic examination was otherwise normal.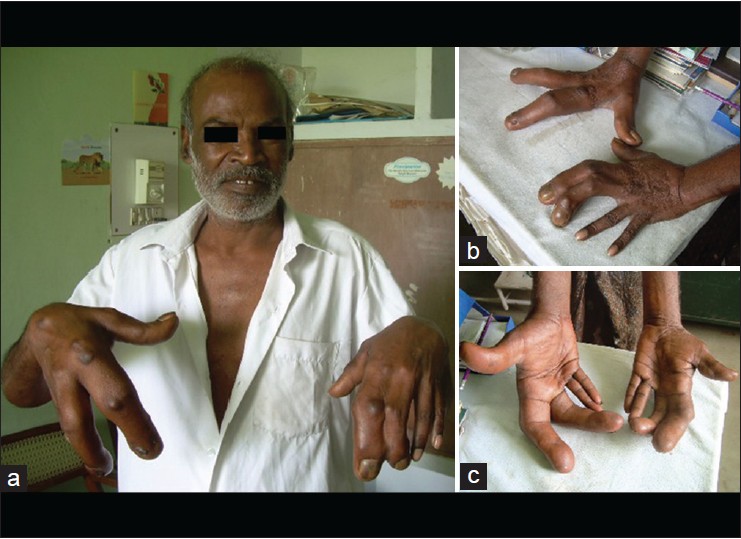 | Figure 1: Hypertrophy of index and middle finger of both the hand (a,b,c) and thumb of the right hand (c)
Click here to view |
Laboratory investigations revealed normal renal and liver function tests. His X-ray of hands showed hyperostosis of involved fingers [Figure 2]. The chest X-ray and other skeletal survey were normal. | Figure 2: X - ray hands showing hyperostosis of both index and middle fingure (a,b) and thumb of right hand (b)
Click here to view |
| Discussion | | |
Cohen and Hayden [2] first described this disease in 1979. The name Proteus comes from the Greek god 'Proteus' who had the ability to change his shape and was proposed by Wiedemann, et al. [3] in 1983.
The exact cause of PS remains unclear till date. Happle, et al.[4] in 1987 hypothesized that the syndrome might be due to somatic alteration of a gene leading to mosaic effects that would be lethal if the mutation were carried in nonmosaic fashion. The dysregulated tissue growth in mosaic pattern results in various phenotypic presentations and hence the clinical manifestations of PS are highly variable. [5]
The tissue overgrowth is usually absent or mild at birth and progressive in nature but usually appears to plateau after adolescence. [5] The disproportionate overgrowth of tissue is usually asymmetrical and involves the arms, legs, hands, feet, and digits. Characteristic manifestations include hyperostoses, often near epiphyses with associated impaired mobility and cerebriform connective tissue nevus seen most commonly on plantar surface. Other findings are lipomas, epidermal nevi and capillary vascular malformations [Table 1].
There is no specific molecular marker, or laboratory test, for the diagnosis of PS. The diagnosis is mainly based on history, clinical examination and imaging studies. The proposed criterion for the diagnosis of PS is shown in [Table 1].
Because of its variable presentation, PS may be confused with other conditions. The two disorders most commonly confused with PS are Klippel-Trenaunay syndrome and hemihyperplasia/lipomatosis syndrome. [6] The others being those listed in [Table 2]. The important points in PS that help in the differential diagnosis are:
- Sporadic and progressive nature of tissue overgrowth
- The absent or mild tissue growth at birth
- Absence of bone tumor, enchondromas
- Absence of specific gene mutations differentiates from neurofibromatosis
- Absence of familial inheritance (postzygotic somatic mutation of genes)
There are no effective treatment modalities for PS. The patients should be followed up regularly for development of complications and their management. The management is also challenging because of progressive nature of tissue growth. Both benign and malignant tumors are associated with PS. [7] Two relatively common tumors include cystadenomas of the ovary and monomorphic adenomas of the parotid gland. The patients are also at risk of developing psychological and social problems.
Our patient presented with macrodactyly of index and middle finger of both the hands and thumb of right hand (one criteria of category B) and he met all the three general criteria. His skeletal survey was normal except for hyperostosis of index and middle finger and there were no associated complications except for the limitation of his affected finger movements. Although the patient did not satisfy the proposed criteria [Table 1], a literature search revealed that out of the 205 cases reported 90 satisfied the criteria highlighting the variability in clinical presentation in cases of PS. [6]
Our patient was managed as a case of inferior wall MI and is presently on anti-ischemic medications with no new complications.
In conclusion, PS is a very rare and highly variable, progressive tissue overgrowth disorder. Patients should be kept under regular follow-up for the development of complications and their management.
| References | | |
| 1. | Biesecker LG. Multifaceted challenges of proteus syndrome. JAMA 2001;285:2240-3. 
[PUBMED] |
| 2. | Cohen MM Jr, Hayden PW. A newly recognized hamartomatous syndrome. Birth Defects Orig Artic Ser 1979;15:291-6.
[PUBMED] |
| 3. | Wiedemann HR, Burgio GR, Aldenhoff P, Kunze J, Kaufmann HJ, Schirg E, et al. The Proteus syndrome: partial gigantism of the hands and/or feet, nevi, hemihypertrophy, subcutaneous tumors, macrocephaly, or other skull anomalies and possible accelerated growth and visceral affections. Eur J Pediatr 1983;140:5-12.
|
| 4. | Happle R. Lethal genes surviving by mosaicism: A possible explanation for sporadic birth defects involving the skin. J Am Acad Dermatol 1987;16:899-906.
[PUBMED] |
| 5. | Cohen MM Jr. Proteus syndrome: Clinical evidence for somatic mosaicism and selective review. Am J Med Genet 1993;47:645-52.
[PUBMED] |
| 6. | Biesecker LG, Happle R, Mulliken JB, Weksberg R, Graham JM Jr, Viljoen DL, et al. Proteus Syndrome: Diagnostic Criteria, Differential Diagnosis, and Patient Evaluation. Am J Med Genet 1999;84:389-95.
[PUBMED] |
| 7. | Gordon PL, Wilroy RS, Lasater OE, Cohen MM Jr. Neoplasms in Proteus syndrome. Am J Med Genet 1995;57:74-8.
[PUBMED] |
[Figure 1], [Figure 2]
[Table 1], [Table 2]
|